

Early fluid resuscitation reduces morbidity among patients with acute pancreatitis
- PMID: 21554987
- PMCID: PMC3143229
- DOI: 10.1016/j.cgh.2011.03.032
Early fluid resuscitation reduces morbidity among patients with acute pancreatitis
Abstract
Background & aims: Early fluid resuscitation is recommended to reduce morbidity and mortality among patients with acute pancreatitis, although the impact of this intervention has not been quantified. We investigated the association between early fluid resuscitation and outcome of patients admitted to the hospital with acute pancreatitis.
Methods: Nontransfer patients admitted to our center with acute pancreatitis from 1985-2009 were identified retrospectively. Patients were stratified into groups on the basis of early (n = 340) or late resuscitation (n = 94). Early resuscitation was defined as receiving ≥one-third of the total 72-hour fluid volume within 24 hours of presentation, whereas late resuscitation was defined as receiving ≤one-third of the total 72-hour fluid volume within 24 hours of presentation. The primary outcomes were frequency of systemic inflammatory response syndrome (SIRS), organ failure, and death.
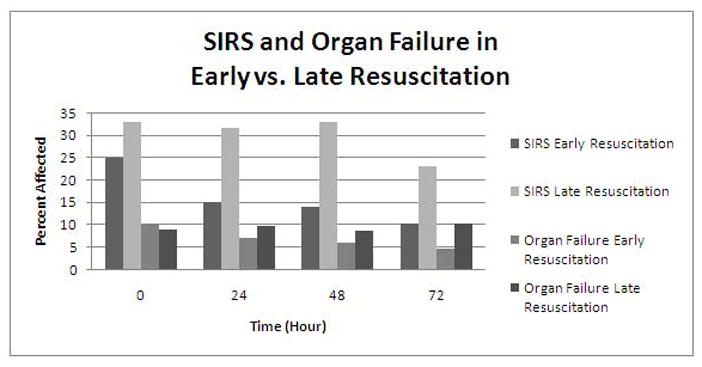
Results: Early resuscitation was associated with decreased SIRS, compared with late resuscitation, at 24 hours (15% vs 32%, P = .001), 48 hours (14% vs 33%, P = .001), and 72 hours (10% vs 23%, P = .01), as well as reduced organ failure at 72 hours (5% vs 10%, P < .05), a lower rate of admission to the intensive care unit (6% vs 17%, P < .001), and a reduced length of hospital stay (8 vs 11 days, P = .01). Subgroup analysis demonstrated that these benefits were more pronounced in patients with interstitial rather than severe pancreatitis at admission.
Conclusions: In patients with acute pancreatitis, early fluid resuscitation was associated with reduced incidence of SIRS and organ failure at 72 hours. These effects were most pronounced in patients admitted with interstitial rather than severe disease.
Copyright © 2011 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Early fluid resuscitation in acute pancreatitis: a lot more than just fluids.Clin Gastroenterol Hepatol. 2011 Aug;9(8):633-4. doi: 10.1016/j.cgh.2011.03.010. Epub 2011 Mar 21. Clin Gastroenterol Hepatol. 2011. PMID: 21421079 No abstract available.
-
The dynamic nature of fluid resuscitation in acute pancreatitis.Clin Gastroenterol Hepatol. 2012 Jan;10(1):95-6; author reply 96. doi: 10.1016/j.cgh.2011.08.020. Epub 2011 Aug 31. Clin Gastroenterol Hepatol. 2012. PMID: 21888883 No abstract available.
References
-
- Swaroop VS, Chari ST, Clain JE. Severe acute pancreatitis. JAMA. 2004;291:2865–2868. - PubMed
-
- Banks PA, Freeman ML. Practice Parameters Committee of the American College of G. Practice guidelines in acute pancreatitis. American Journal of Gastroenterology. 2006;101(10):2379–2400. - PubMed
-
- Fagenholz PJ, Fernandez-Del Castillo C, Harris NS, Pelletier AJ, Camargo CA. Increasing United States Hospital Admissions for Acute Pancreatitis, 1988–2003. Annals of Epidemiology. 2007;17(7):491–498. - PubMed
-
- Fagenholz PJ, Fernandez-Del Castillo C, Harris NS, Pelletier AJ, Camargo CA. Direct medical costs of acute pancreatitis hospitalizations in the United States. Pancreas. 2007;35(4):302–307. - PubMed
-
- Forsmark CE, Baillie J. AGA Institute technical review on acute pancreatitis. Gastroenterology. 2007;132(5):2022–2044. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
