

Long-term outcomes following positive fecal occult blood test results in older adults: benefits and burdens
- PMID: 21555655
- PMCID: PMC3291514
- DOI: 10.1001/archinternmed.2011.206
Long-term outcomes following positive fecal occult blood test results in older adults: benefits and burdens
Abstract
Background: In the United States, older adults have low rates of follow-up colonoscopy after a positive fecal occult blood test (FOBT) result. The long-term outcomes of these real world practices and their associated benefits and burdens are unknown.
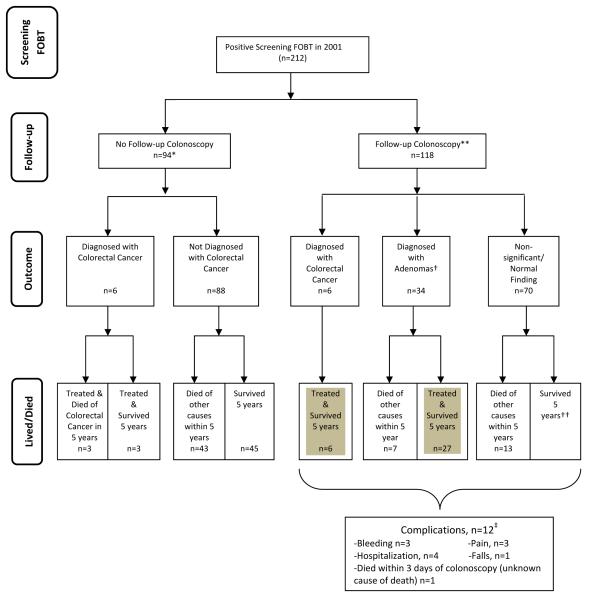
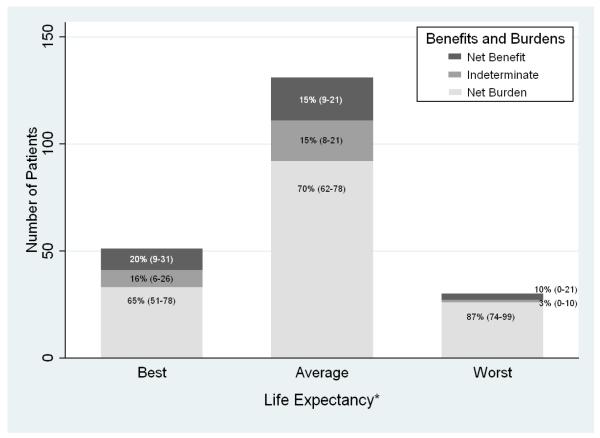
Methods: Longitudinal cohort study of 212 patients 70 years or older with a positive FOBT result at 4 Veteran Affairs (VA) facilities in 2001 and followed up through 2008. We determined the frequency of downstream outcomes during the 7 years of follow-up, including procedures, colonoscopic findings, outcomes of treatment, complications, and mortality based on chart review and national VA and Medicare data. Net burden or benefit from screening and follow-up was determined according to each patient's life expectancy. Life expectancy was classified into 3 categories: best (age, 70-79 years and Charlson-Deyo comorbidity index [CCI], 0), average, and worst (age, 70-84 years and CCI, ≥4 or age, ≥85 years and CCI, ≥1).
Results: Fifty-six percent of patients received follow-up colonoscopy (118 of 212), which found 34 significant adenomas and 6 cancers. Ten percent experienced complications from colonoscopy or cancer treatment (12 of 118). Forty-six percent of those without follow-up colonoscopy died of other causes within 5 years of FOBT (43 of 94), while 3 died of colorectal cancer within 5 years. Eighty-seven percent of patients with worst life expectancy experienced a net burden from screening (26 of 30) as did 70% with average life expectancy (92 of 131) and 65% with best life expectancy (35 of 51) (P = .048 for trend).
Conclusions: Over a 7-year period, older adults with best life expectancy were less likely to experience a net burden from current screening and follow-up practices than are those with worst life expectancy. The net burden could be decreased by better targeting FOBT screening and follow-up to healthy older adults.
Figures
Comment in
-
Colorectal cancer screening protocols and procedures: comment on "Overuse of screening colonoscopy in the Medicare population" and "Long-term outcomes following positive fecal occult blood test results in older adults".Arch Intern Med. 2011 Aug 8;171(15):1351. doi: 10.1001/archinternmed.2011.198. Epub 2011 May 9. Arch Intern Med. 2011. PMID: 21555652 No abstract available.
-
Screening for colorectal cancer in the elderly population: how much is enough?Arch Intern Med. 2011 Aug 8;171(15):1332-4. doi: 10.1001/archinternmed.2011.364. Arch Intern Med. 2011. PMID: 21824947 No abstract available.
Similar articles
-
Lack of follow-up after fecal occult blood testing in older adults: inappropriate screening or failure to follow up?Arch Intern Med. 2011 Feb 14;171(3):249-56. doi: 10.1001/archinternmed.2010.372. Epub 2010 Oct 11. Arch Intern Med. 2011. PMID: 20937917 Free PMC article.
-
Fecal occult blood test for colorectal cancer screening: an evidence-based analysis.Ont Health Technol Assess Ser. 2009;9(10):1-40. Epub 2009 Sep 1. Ont Health Technol Assess Ser. 2009. PMID: 23074514 Free PMC article.
-
Rates and correlates of potentially inappropriate colorectal cancer screening in the Veterans Health Administration.J Gen Intern Med. 2015 Jun;30(6):732-41. doi: 10.1007/s11606-014-3163-8. Epub 2015 Jan 21. J Gen Intern Med. 2015. PMID: 25605531 Free PMC article.
-
Screening for Colorectal Cancer: An Updated Systematic Review [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2008 Oct. Report No.: 08-05-05124-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2008 Oct. Report No.: 08-05-05124-EF-1. PMID: 20722162 Free Books & Documents. Review.
-
The compliance rate for the second diagnostic evaluation after a positive fecal occult blood test: A systematic review and meta-analysis.United European Gastroenterol J. 2019 Apr;7(3):424-448. doi: 10.1177/2050640619828185. Epub 2019 Feb 6. United European Gastroenterol J. 2019. PMID: 31019712 Free PMC article.
Cited by
-
Fecal immunochemical test for colorectal cancer from a prospective cohort with 513,283 individuals: Providing detailed number needed to scope (NNS) before colonoscopy.Medicine (Baltimore). 2016 Sep;95(36):e4414. doi: 10.1097/MD.0000000000004414. Medicine (Baltimore). 2016. PMID: 27603337 Free PMC article.
-
Physician decision making for colorectal cancer screening in the elderly.J Gen Intern Med. 2013 Sep;28(9):1202-7. doi: 10.1007/s11606-013-2393-5. Epub 2013 Mar 29. J Gen Intern Med. 2013. PMID: 23539281 Free PMC article.
-
Improving hepatocellular carcinoma screening: applying lessons from colorectal cancer screening.Clin Gastroenterol Hepatol. 2013 May;11(5):472-7. doi: 10.1016/j.cgh.2012.11.010. Epub 2012 Nov 28. Clin Gastroenterol Hepatol. 2013. PMID: 23200983 Free PMC article.
-
Influence of Age, Health, and Function on Cancer Screening in Older Adults with Limited Life Expectancy.J Gen Intern Med. 2019 Jan;34(1):110-117. doi: 10.1007/s11606-018-4717-y. Epub 2018 Nov 6. J Gen Intern Med. 2019. PMID: 30402822 Free PMC article.
-
Colorectal Cancer Screening and Surveillance Colonoscopy in Older Adults.Curr Treat Options Gastroenterol. 2019 Jun;17(2):292-302. doi: 10.1007/s11938-019-00230-9. Curr Treat Options Gastroenterol. 2019. PMID: 30969399 Free PMC article. Review.
References
-
- Levin B, Hess K, Johnson C. Screening for colorectal cancer. A comparison of 3 fecal occult blood tests. Arch Intern Med. 1997 May 12;157(9):970–976. - PubMed
-
- Lurie JD, Welch HG. Diagnostic testing following fecal occult blood screening in the elderly. J Natl Cancer Inst. 1999 Oct 6;91(19):1641–1646. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
