

Time trends in pulmonary embolism in the United States: evidence of overdiagnosis
- PMID: 21555660
- PMCID: PMC3140219
- DOI: 10.1001/archinternmed.2011.178
Time trends in pulmonary embolism in the United States: evidence of overdiagnosis
Abstract
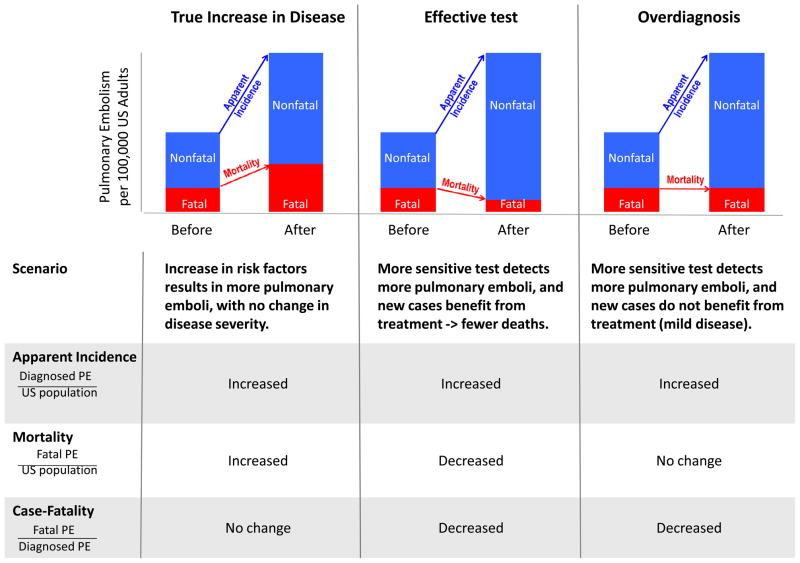
Background: Computed tomographic pulmonary angiography (CTPA) may improve detection of life-threatening pulmonary embolism (PE), but this sensitive test may have a downside: overdiagnosis and overtreatment (finding clinically unimportant emboli and exposing patients to harms from unnecessary treatment).
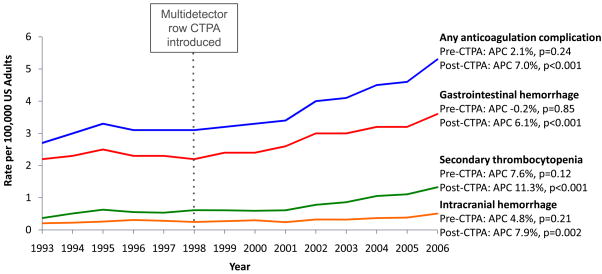
Methods: To assess the impact of CTPA on national PE incidence, mortality, and treatment complications, we conducted a time trend analysis using the Nationwide Inpatient Sample and Multiple Cause-of-Death databases. We compared age-adjusted incidence, mortality, and treatment complications (in-hospital gastrointestinal tract or intracranial hemorrhage or secondary thrombocytopenia) of PE among US adults before (1993-1998) and after (1998-2006) CTPA was introduced.
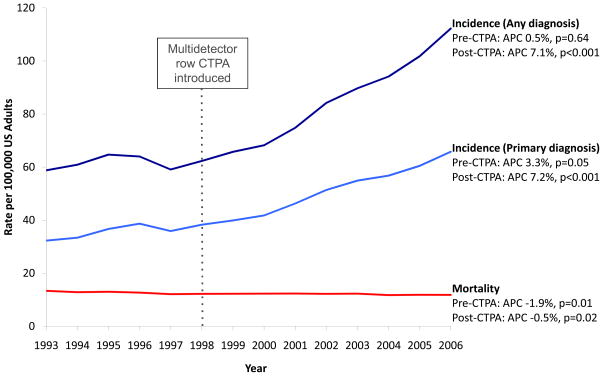
Results: Pulmonary embolism incidence was unchanged before CTPA (P = .64) but increased substantially after CTPA (81% increase, from 62.1 to 112.3 per 100,000; P < .001). Pulmonary embolism mortality decreased during both periods: more so before CTPA (8% reduction, from 13.4 to 12.3 per 100,000; P < .001) than after (3% reduction, from 12.3 to 11.9 per 100,000; P = .02). Case fatality improved slightly before (8% decrease, from 13.2% to 12.1%; P = .02) and substantially after CTPA (36% decrease, from 12.1% to 7.8%; P < .001). Meanwhile, CTPA was associated with an increase in presumed complications of anticoagulation for PE: before CTPA, the complication rate was stable (P = .24), but after it increased by 71% (from 3.1 to 5.3 per 100,000; P < .001).
Conclusions: The introduction of CTPA was associated with changes consistent with overdiagnosis: rising incidence, minimal change in mortality, and lower case fatality. Better technology allows us to diagnose more emboli, but to minimize harms of overdiagnosis we must learn which ones matter.
Figures
Comment in
-
Acute pulmonary embolism: comment on "time trends in pulmonary embolism in the United States".Arch Intern Med. 2011 May 9;171(9):837-9. doi: 10.1001/archinternmed.2011.174. Arch Intern Med. 2011. PMID: 21555661 No abstract available.
-
Caution on interpreting the time trends in pulmonary embolism as "overdiagnosis".Arch Intern Med. 2011 Nov 28;171(21):1962; author reply 1962-3. doi: 10.1001/archinternmed.2011.549. Arch Intern Med. 2011. PMID: 22123814 No abstract available.
References
-
- Wittram C, Meehan MJ, Halpern EF, Shepard JA, McLoud TC, Thrall JH. Trends in thoracic radiology over a decade at a large academic medical center. J Thorac Imaging. 2004;19(3):164–170. - PubMed
-
- Donohoo JH, Mayo-Smith WW, Pezzullo JA, Egglin TK. Utilization patterns and diagnostic yield of 3421 consecutive multidetector row computed tomography pulmonary angiograms in a busy emergency department. J Comput Assist Tomogr. 2008;32(3):421–425. - PubMed
-
- Weir ID, Drescher F, Cousin D, et al. Trends in use and yield of chest computed tomography with angiography for diagnosis of pulmonary embolism in a Connecticut hospital emergency department. Conn Med. 2010;74(1):5–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
