

Racial differences in primary care opioid risk reduction strategies
- PMID: 21555749
- PMCID: PMC3090430
- DOI: 10.1370/afm.1242
Racial differences in primary care opioid risk reduction strategies
Abstract
Purpose: Racial disparities in treating pain with opioids are widely reported; however, differences in use of recommended strategies to reduce the risk of opioid misuse by race/ethnicity have not been evaluated.
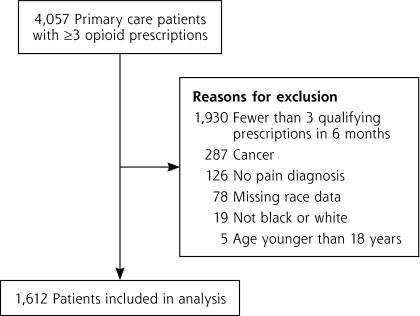
Methods: In a retrospective cohort of black and white patients with chronic noncancer pain prescribed opioid analgesics for at least 3 months, we assessed physicians' use of 3 opioid risk reduction strategies: (1) urine drug testing, (2) regular office visits (at least 1 visit per 6 months on opioids and within 30 days of an opioid change), and (3) restricted early opioid refills (receipt of a refill >1 week early less than twice). Nonlinear mixed effect regression models accounted for clustering within physician and adjusted additively for demographics, substance abuse, mental health and medical comorbidities, health care factors, and practice site.
Results: Of the 1,612 patients studied, 62.1% were black. Black patients were more likely than white patients to receive urine drug testing (10.4% vs 4.1%), regular office visits (56.4% vs 39.0%), and restricted early refills (79.4% vs 72.0%) (P <.001 for each). In fully adjusted models, black patients had significantly higher odds than their white counterparts of receiving regular office visits (odds ratio = 1.51; 95% confidence interval, 1.06-2.14) and restricted early refills (odds ratio = 1.55; 95% confidence interval, 1.03-2.32), but not urine drug testing (odds ratio = 1.41; 95% confidence interval, 0.78-2.54).
Conclusions: In this cohort of primary care patients receiving opioid analgesics on a long-term basis, use of risk reduction strategies was very limited overall; however, black patients were more likely than white patients to receive 2 of 3 guideline-recommended strategies. These data raise questions about lax monitoring, especially for white patients taking opioids long term.
References
-
- Olsen Y, Daumit GL, Ford DE. Opioid prescriptions by U.S. primary care physicians from 1992 to 2001. J Pain. 2006;7(4):225–235. - PubMed
-
- Pletcher MJ, Kertesz SG, Kohn MA, Gonzales R. Trends in opioid prescribing by race/ethnicity for patients seeking care in US emergency departments. JAMA. 2008;299(1):70–78. - PubMed
-
- Tamayo-Sarver JH, Dawson NV, Hinze SW, et al. The effect of race/ethnicity and desirable social characteristics on physicians’ decisions to prescribe opioid analgesics. Acad Emerg Med. 2003;10(11):1239–1248. - PubMed
-
- Becker WC, Sullivan LE, Tetrault JM, Desai RA, Fiellin DA. Non-medical use, abuse and dependence on prescription opioids among U.S. adults: psychiatric, medical and substance use correlates. Drug Alcohol Depend. 2008;94(1–3):38–47. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous