

Maternal outcomes after HAART for the prevention of mother-to-child transmission in HIV-infected women in Brazil
- PMID: 21555817
- PMCID: PMC3437753
- DOI: 10.3851/IMP1779
Maternal outcomes after HAART for the prevention of mother-to-child transmission in HIV-infected women in Brazil
Abstract
Background: Information is lacking on outcomes in HIV-infected Brazilian women with CD4(+) T-cell counts >200 cells/mm(3) who initiate HAART for the prevention of mother-to-child transmission, and discontinue after delivery.
Methods: Clinical event rates after postpartum HAART discontinuation were calculated for all WHO stage 2-3 events, as well as for HIV progression warranting HAART re-initiation, defined by a WHO stage 4 event and/or CD4(+) T-cell decrease to ≤200 cells/mm(3). Predictors of the WHO stage 2-3 events and HIV progression outcomes were evaluated with Cox's proportional hazards models.
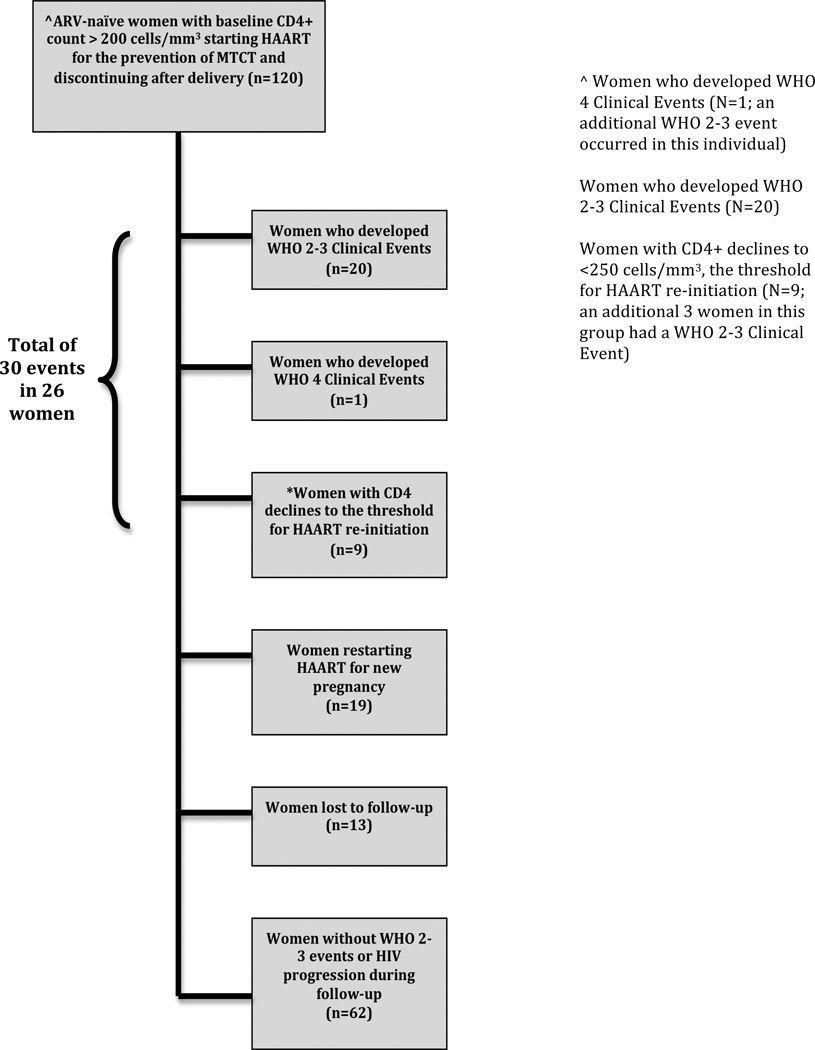
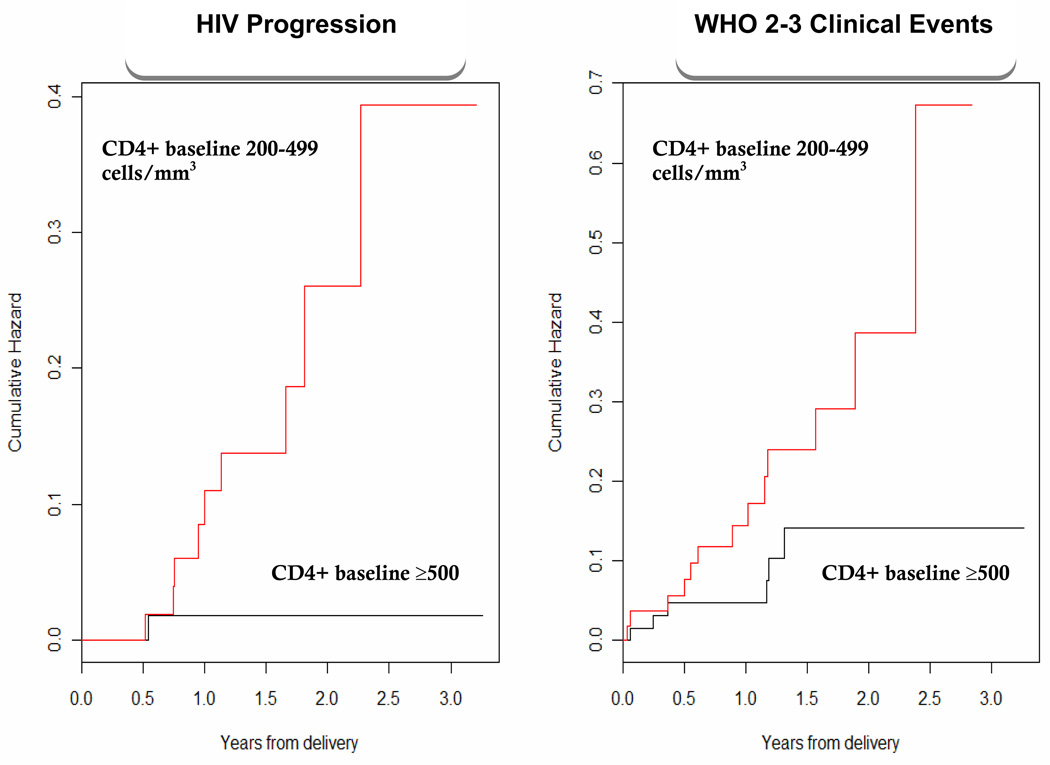
Results: A total of 120 women were followed for a mean of 1.5 years after delivery. Overall, 26 women had 30 events as follows: 20 developed WHO stage 2-3 events, yielding an incidence rate of 13/100 person-years (PY; 95% CI 8-20); 10 developed HIV progression requiring HAART re-initiation (incidence ratio 6/100 PY, 95% CI 3-11). Among progressors, a single woman developed a WHO stage 4 clinical event and the remainder had CD4(+) T-cell decreases. Women who had baseline CD4(+) T-cell counts between 200-500 cells/mm(3) had a hazard ratio for WHO stage 2-3 events of 2.5 compared to women with baseline ≥500 cells/mm(3) (95% CI 1.0-6.3; P=0.05). The only significant predictor of HIV progression was baseline CD4(+) T-cell count (hazard ratio 0.99, 95% CI 0.98-0.99; P=0.02).
Conclusions: In this observational study, a baseline CD4(+) T-cell count <500 cells/mm(3) was associated with an increased risk of postpartum WHO stage 2-3 clinical events and HIV disease progression. Randomized studies are needed to further evaluate the effect of postpartum treatment discontinuation on maternal health.
Figures
References
-
- Cooper ER, Charurat M, Mofenson L, et al. Combination antiretroviral strategies for the treatment of pregnant HIV-1-infected women and prevention of perinatal HIV-1 transmission. J Acquir Immune Defic Syndr. 2002 Apr 15;29(5):484–494. - PubMed
-
- STI UWWGoGHAa, editor. UNAIDS Joint United Nations Programme on HIV/AIDS Country Report: Brazil. Geneva, Switzerland: UNAIDS; 2008.
-
- Ministry of Health B, editor. Recomendações para profilaxia da transmissão vertical do HIV e terapia anti-retroviral em gestantes / Ministério da Saúde, Secretaria de Vigilância em Saúde. 2006
-
- El-Sadr WM, Lundgren JD, Neaton JD, et al. CD4+ count-guided interruption of antiretroviral treatment. N Engl J Med. 2006 Nov 30;355(22):2283–2296. - PubMed
-
- WHO . In: WHO Case Definitions of HIV for Surveillance and Revised Clinical Staging and Immunological Classification of HIV-Related Disease in Adults and Children. Program HA, editor. Geneva: 2007.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
