

A comparison of obstetric maneuvers for the acute management of shoulder dystocia
- PMID: 21555962
- PMCID: PMC3101300
- DOI: 10.1097/AOG.0b013e31821a12c9
A comparison of obstetric maneuvers for the acute management of shoulder dystocia
Abstract
Objective: To assess the efficacy of obstetric maneuvers for resolving shoulder dystocia and the effect that these maneuvers have on neonatal injury when shoulder dystocia occurs.
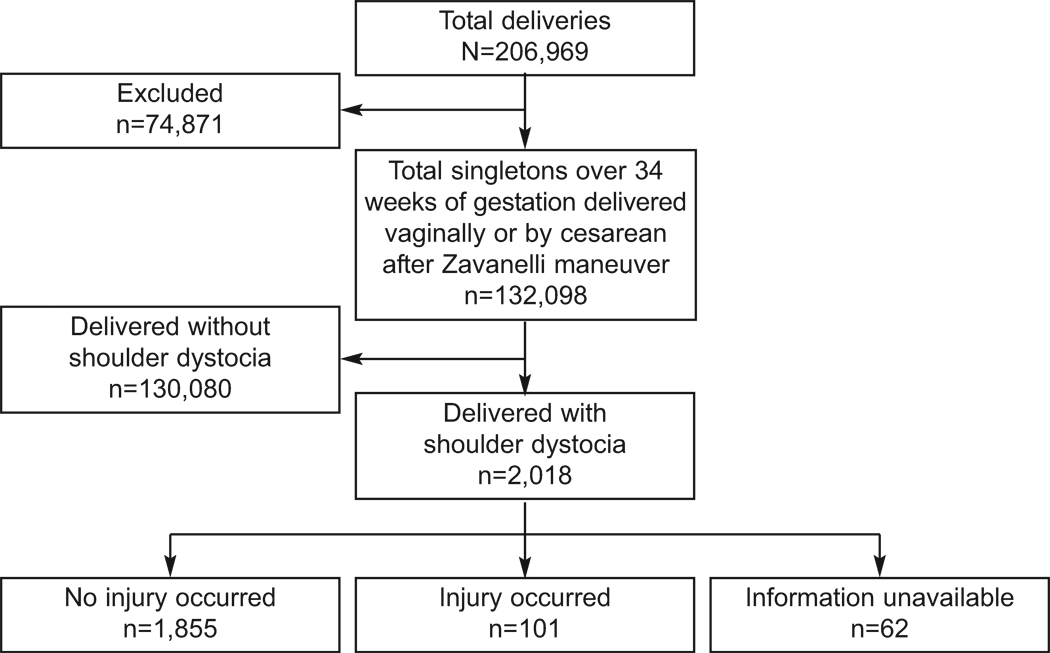
Methods: Using an electronic database encompassing 206,969 deliveries, we identified all women with a vertex fetus beyond 34 0/7 weeks of gestation who incurred a shoulder dystocia during the process of delivery. Women whose fetuses had a congenital anomaly and women with an antepartum stillbirth were excluded. Medical records of all cases were reviewed by trained abstractors. Cases involving neonatal injury (defined as brachial plexus injury, clavicular or humerus fracture, or hypoxic-ischemic encephalopathy or intrapartum neonatal death attributed to the shoulder dystocia) were compared with those without injury.
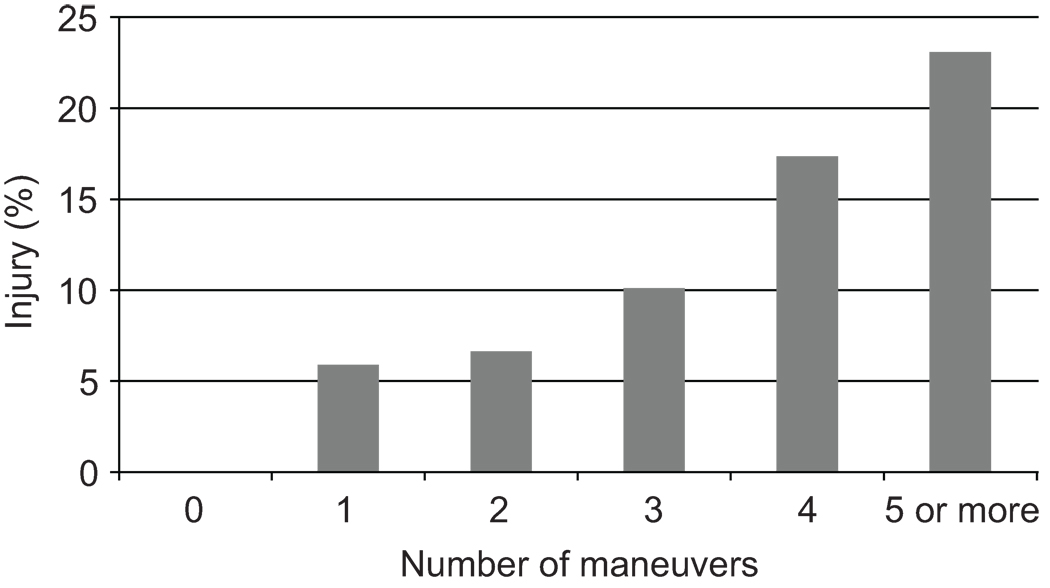
Results: Among 132,098 women who delivered a term cephalic liveborn fetus vaginally, 2,018 incurred a shoulder dystocia (1.5%), and 101 (5.2%) of these incurred a neonatal injury. Delivery of the posterior shoulder was associated with the highest rate of delivery when compared with other maneuvers (84.4% compared with 24.3-72.0% for other maneuvers; P<.005 to P<.001) and similar rates of neonatal injury (8.4% compared with 6.1-14.0%; P=.23 to P=.7). The total number of maneuvers performed significantly correlated with the rate of neonatal injury (P<.001).
Conclusion: Delivery of the posterior shoulder should be considered following the McRoberts maneuver and suprapubic pressure in the management of shoulder dystocia. The need for additional maneuvers was associated with higher rates of neonatal injury.
Conflict of interest statement
Figures
Comment in
-
A comparison of obstetric maneuvers for the acute management of shoulder dystocia.Obstet Gynecol. 2012 Feb;119(2 Pt 1):386; author reply 386-7. doi: 10.1097/AOG.0b013e318244b405. Obstet Gynecol. 2012. PMID: 22270305 No abstract available.
References
-
- ACOG Committee on Practice Bulletins-Gynecology, The American College of Obstetrician and Gynecologists. ACOG practice bulletin clinical management guidelines for obstetrician-gynecologists. number 40, november 2002. Obstet Gynecol. 2002 Nov;100(5 Pt 1):1045–1050. - PubMed
-
- Gherman RB, Goodwin TM, Souter I, Neumann K, Ouzounian JG, Paul RH. The McRoberts' maneuver for the alleviation of shoulder dystocia: How successful is it? Am J Obstet Gynecol. 1997 Mar;176(3):656–661. - PubMed
-
- Mavroforou A, Koumantakis E, Michalodimitrakis E. Physicians' liability in obstetric and gynecology practice. Med Law. 2005 Mar;24(1):1–9. - PubMed
-
- Lewis DF, Edwards MS, Asrat T, Adair CD, Brooks G, London S. Can shoulder dystocia be predicted? preconceptive and prenatal factors. J Reprod Med. 1998 Aug;43(8):654–658. - PubMed
-
- Mazouni C, Porcu G, Cohen-Solal E, Heckenroth H, Guidicelli B, Bonnier P, et al. Maternal and anthropomorphic risk factors for shoulder dystocia. Acta Obstet Gynecol Scand. 2006;85(5):567–570. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
