

Endoscope-assisted microsurgical transoral approach to the anterior craniovertebral junction compressive pathologies
- PMID: 21556730
- PMCID: PMC3175898
- DOI: 10.1007/s00586-011-1769-7
Endoscope-assisted microsurgical transoral approach to the anterior craniovertebral junction compressive pathologies
Abstract
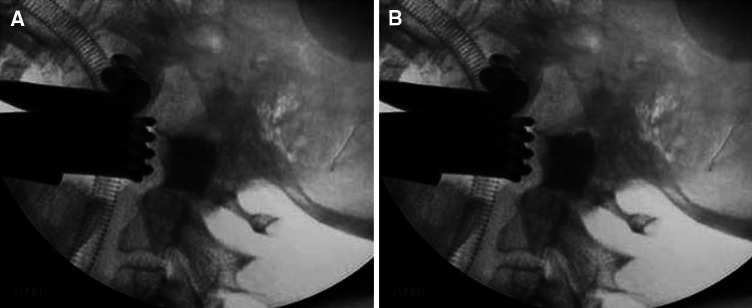
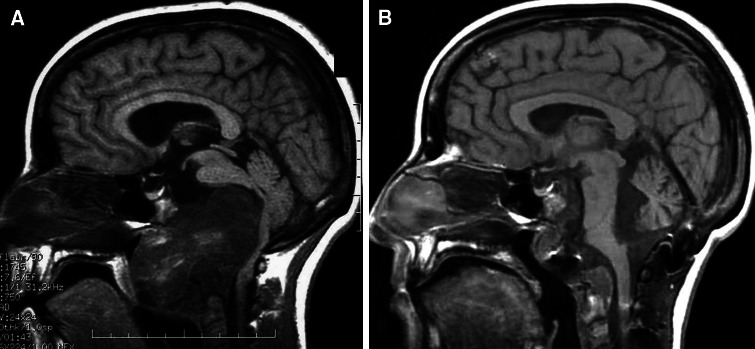
At the present time, an update to the classical microsurgical transoral decompression is strongly provided by the most recent literature dealing with the introduction of the endoscopy in spine surgery. In this paper, we present our experience on the endoscope-assisted microsurgical transoral approach to anterior craniovertebral junction (CVJ) compressive pathology. We analysed seven patients (3 paediatrics and 4 adults ranging from 6 to 78 years) operated on for CVJ decompressive procedures using an open access, microsurgical technique, neuronavigation and endoscopy. All techniques mentioned were simultaneously employed. Among the endoscopic routes described in the literature, we have preferred the transoral using 30° endoscopes. In all the cases endoscopy allowed a radical decompression compared to the microsurgical technique alone, as confirmed intraoperatively with contrast medium fluoroscopy. In conclusion, endoscopy represents a useful complement to the standard microsurgical approach to the anterior CVJ; it provides information for a better decompression with no need for soft palate splitting, hard palate resection, or extended maxillotomy. Moreover, intraoperative fluoroscopy helps to recognize residual compression. Virtually, in normal anatomic conditions, no surgical limitations exist for endoscopically assisted transoral approach, compared with the pure endonasal and transcervical endoscopic approaches. In our opinion, the endoscope deserves a role as "support" to the standard transoral microsurgical approach since 30° angulated endoscopy significantly increases the surgical area exposed at the level of the anterior CVJ.
Figures



References
-
- Menezes A. Occipito-cervical fusion: indications, technique and avoidance of complications. In: Hitchon P, editor. Techniques of spinal fusion and stabilisation. New York: Thieme; 1994. pp. 82–91.
-
- Visocchi M, Di Rocco F, Meglio M (2003) Craniocervical junction instability: instrumentation and fusion with titanium rods and sublaminar wires. Effectiveness and failures in personal experience. Acta Neurochir (Wien) 145:265–272 (discussion 272). doi:10.1007/s00701-002-1067-6 - PubMed
-
- Visocchi M, Cabezas DC, Rocco CD, Meglio M (2001) Craniocervical instability, instrumentation and fusion: personal experience with contoured titanium bar and sublaminar wires. In: Culloch GM, Reilly P (eds) World Federation of Neurosurgical Societies 12th World Congress of Neurosurgery. Sydney Australia, pp 279–283
-
- Sonntag W, Dickman C. Posterior occipital C1–C2 instrumentation. In: Menezes A, editor. Principles of spinal surgery. New York: McGraw Hill; 1996. pp. 1067–1079.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
