

Implementation of a fast-track clinical pathway decreases postoperative length of stay and hospital charges for liver resection
- PMID: 21556940
- PMCID: PMC3210369
- DOI: 10.1007/s12013-011-9203-7
Implementation of a fast-track clinical pathway decreases postoperative length of stay and hospital charges for liver resection
Abstract
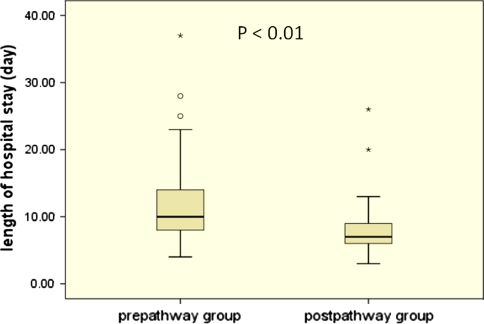
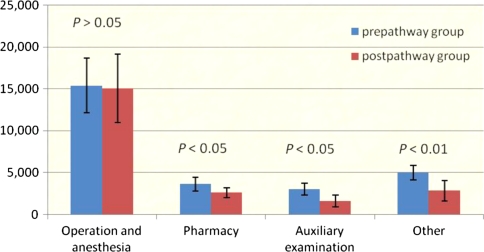
A fast-track clinical pathway is designed to streamline patient care delivery and maximize cost effectiveness. It has decreased postoperative length of stay (LOS) and hospital charges for many surgical procedures. However, data on clinical pathways after liver surgery are sparse. This study examined whether use of a fast-track clinical pathway for patients undergoing elective liver resection affected postoperative LOS and hospital charges. A fast-track clinical pathway was developed and implemented by a multidisciplinary team for patients undergoing liver resection. Between July, 2007 and May, 2008, a total of 117 patients underwent elective liver resection: the fast-track clinical pathway (education of patients and families, earlier oral feeding, earlier discontinuation of intravenous fluid, no drains or nasogastric tubes, early ambulation, use of a urinary catheter for less than 24 h and planned discharge 6 days after surgery) was studied prospectively in 56 patients (postpathway group). These patients were compared with the remainder who had usual care (prepathway group). Outcome measures were postoperative LOS, perioperative hospital charges, intraoperative and postoperative complications, mortality, and readmission rate. Among all patients, 69 (59%) had complicating diseases and/or a history of surgery and 24 patients belonged to American Society of Anesthesiologists grade III-IV. Compared with the prepathway group, the postpathway group had a significantly shorter postoperative LOS (7 vs. 11 days, P < 0.01). The average perioperative hospital charges were RMB 26,626 for patients in the prepathway group and only RMB 21,004 for those in the postpathway group (P < 0.05), with no differences in intraoperative and postoperative complications (P = 0.814), mortality (P = 0.606), and readmission rate (P = 0.424). Implementation of the fast-track clinical pathway is an effective and safe method for reducing postoperative LOS and hospital charges for high-risk patients undergoing elective liver resection. The result supports the further development of fast-track clinical pathways for liver surgical procedures.
Figures
References
-
- Coffey RJ, Richards JS, Remmert CS, LeRoy SS, Schoville RR, Baldwin PJ. An introduction to critical paths. Quality Management in Health Care. 1992;1(1):45–54. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
