

Can an electronic prescribing system detect doctors who are more likely to make a serious prescribing error?
- PMID: 21558099
- PMCID: PMC3089874
- DOI: 10.1258/jrsm.2011.110061
Can an electronic prescribing system detect doctors who are more likely to make a serious prescribing error?
Abstract
Objectives: We aimed to assess whether routine data produced by an electronic prescribing system might be useful in identifying doctors at higher risk of making a serious prescribing error.
Design: Retrospective analysis of prescribing by junior doctors over 12 months using an electronic prescribing information and communication system. The system issues a graded series of prescribing alerts (low-level, intermediate, and high-level), and warnings and prompts to respond to abnormal test results. These may be overridden or heeded, except for high-level prescribing alerts, which are indicative of a potentially serious error and impose a 'hard stop'.
Setting: A large teaching hospital.
Participants: All junior doctors in the study setting.
Main outcome measures: Rates of prescribing alerts and laboratory warnings and doctors' responses.
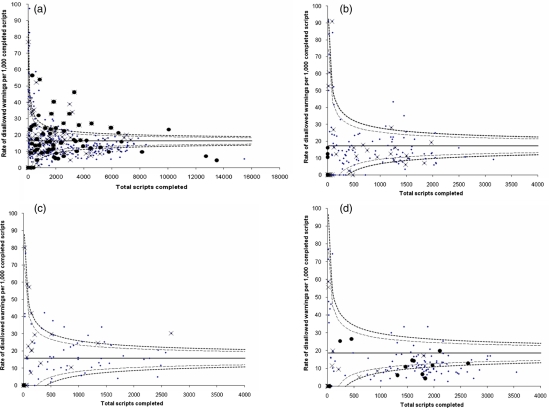
Results: Altogether 848,678 completed prescriptions issued by 381 doctors (median 1538 prescriptions per doctor, interquartile range [IQR] 328-3275) were analysed. We identified 895,029 low-level alerts (median 1033 per 1000 prescriptions per doctor, IQR 903-1205) with a median of 34% (IQR 31-39%) heeded; 172,434 intermediate alerts (median 196 per 1000 prescriptions per doctor, IQR 159-266), with a median of 23% (IQR 16-30%) heeded; and 11,940 high-level 'hard stop' alerts. Doctors vary greatly in the extent to which they trigger and respond to alerts of different types. The rate of high-level alerts showed weak correlation with the rate of intermediate prescribing alerts (correlation coefficient, r = 0.40, P = <0.001); very weak correlation with low-level alerts (r = 0.12, P = 0.019); and showed weak (and sometimes negative) correlation with propensity to heed test-related warnings or alarms. The degree of correlation between generation of intermediate and high-level alerts is insufficient to identify doctors at high risk of making serious errors.
Conclusions: Routine data from an electronic prescribing system should not be used to identify doctors who are at risk of making serious errors. Careful evaluation of the kinds of quality assurance questions for which routine data are suitable will be increasingly valuable.
Figures
Similar articles
-
The effect of provider characteristics on the responses to medication-related decision support alerts.Int J Med Inform. 2015 Sep;84(9):630-9. doi: 10.1016/j.ijmedinf.2015.04.006. Epub 2015 May 9. Int J Med Inform. 2015. PMID: 26004341
-
Making electronic prescribing alerts more effective: scenario-based experimental study in junior doctors.J Am Med Inform Assoc. 2011 Nov-Dec;18(6):789-98. doi: 10.1136/amiajnl-2011-000199. Epub 2011 Aug 11. J Am Med Inform Assoc. 2011. PMID: 21836158 Free PMC article. Clinical Trial.
-
Improving feedback on junior doctors' prescribing errors: mixed-methods evaluation of a quality improvement project.BMJ Qual Saf. 2017 Mar;26(3):240-247. doi: 10.1136/bmjqs-2015-004717. Epub 2016 Apr 4. BMJ Qual Saf. 2017. PMID: 27044881 Free PMC article. Review.
-
Perceived causes of prescribing errors by junior doctors in hospital inpatients: a study from the PROTECT programme.BMJ Qual Saf. 2013 Feb;22(2):97-102. doi: 10.1136/bmjqs-2012-001175. Epub 2012 Oct 30. BMJ Qual Saf. 2013. PMID: 23112288
-
[Good prescription practice for out-patients-quality requirements of prescriptions in Germany].Ther Umsch. 2014 Jun;71(6):317-23. doi: 10.1024/0040-5930/a000519. Ther Umsch. 2014. PMID: 24867346 Review. German.
Cited by
-
Provision of medicines information: the example of the British National Formulary.Br J Clin Pharmacol. 2012 Jun;73(6):934-8. doi: 10.1111/j.1365-2125.2012.04241.x. Br J Clin Pharmacol. 2012. PMID: 22360536 Free PMC article.
-
Prescribing errors in hospital practice.Br J Clin Pharmacol. 2012 Oct;74(4):668-75. doi: 10.1111/j.1365-2125.2012.04313.x. Br J Clin Pharmacol. 2012. PMID: 22554316 Free PMC article. Review.
-
What does a good prescribing induction for the newly qualified doctor look like?Future Healthc J. 2020 Feb;7(Suppl 1):s88-s89. doi: 10.7861/fhj.7.1.s88. Future Healthc J. 2020. PMID: 32455312 Free PMC article. No abstract available.
-
Deriving dose limits for warnings in electronic prescribing systems: statistical analysis of prescription data at University Hospital Birmingham, UK.Drug Saf. 2012 Apr 1;35(4):291-8. doi: 10.2165/11594810-000000000-00000. Drug Saf. 2012. PMID: 22263779
-
Effects of a computerized feedback intervention on safety performance by junior doctors: results from a randomized mixed method study.BMC Med Inform Decis Mak. 2013 Jun 4;13:63. doi: 10.1186/1472-6947-13-63. BMC Med Inform Decis Mak. 2013. PMID: 23734871 Free PMC article. Clinical Trial.
References
-
- Marshall MN, Shekelle P, Davies HTO, Smith PC Public reporting on quality in the United States and the United Kingdom. Health Affairs 2003;22:134–48 - PubMed
-
- Davies H Measuring and reporting the quality of care: issues and evidence from the international research literature. Edinburgh: NHS Quality Improvement Scotland, 2006. See http://www.nhsqis.org.uk/nhsqis/files/Davies%20Paper.pdf
-
- McManus C, Vincent C Selecting and educating safer doctors. : Vincent C, Ennis M, Audley R, Medical Accidents. Oxford: Oxford University Press, 2003
-
- Dornan T, Ashcroft D, Heathfield H, et al. An in depth investigation into causes of prescribing errors by foundation trainees in relation to their medical education – EQUIP Study London: General Medical Council, 2009
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
