

Factors influencing retention in care after starting antiretroviral therapy in a rural South African programme
- PMID: 21559280
- PMCID: PMC3086905
- DOI: 10.1371/journal.pone.0019201
Factors influencing retention in care after starting antiretroviral therapy in a rural South African programme
Abstract
Introduction: The prognosis of patients with HIV in Africa has improved with the widespread use of antiretroviral therapy (ART) but these successes are threatened by low rates of long-term retention in care. There are limited data on predictors of retention in care, particularly from rural sites.
Methods: Prospective cohort analysis of outcome measures in adults from a rural HIV care programme in Madwaleni, Eastern Cape, South Africa. The ART programme operates from Madwaleni hospital and seven primary care feeder clinics with full integration between inpatient and outpatient services. Outreach workers conducted home visits for defaulters.
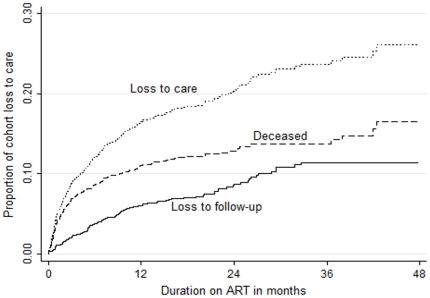
Results: 1803 adults initiated ART from June 2005 to May 2009. At the end of the study period 82.4% were in active care or had transferred elsewhere, 11.1% had died and 6.5% were lost to follow-up (LTFU). Independent predictors associated with an increased risk of LTFU were CD4 nadir >200, initiating ART as an inpatient or while pregnant, and younger age, while being in care for >6 months before initiating ART was associated with a reduced risk. Independent factors associated with an increased risk of mortality were baseline CD4 count <50 and initiating ART as an inpatient, while being in care for >6 months before initiating ART and initiating ART while pregnant were associated with a reduced risk.
Conclusions: Serving a socioeconomically deprived rural population is not a barrier to successful ART delivery. Patients initiating ART while pregnant and inpatients may require additional counselling and support to reduce LTFU. Providing HIV care for patients not yet eligible for ART may be protective against being LTFU and dying after ART initiation.
Conflict of interest statement
Figures
References
-
- Coetzee D, Hildebrand K, Boulle A, Maartens G, Louis F, et al. Outcomes after two years of providing antiretroviral treatment in Khayelitsha, South Africa. AIDS. 2004;18:887. - PubMed
-
- Brodt HR, Kamps BS, Gute P, Knupp B, Staszewski S, Helm EB. Changing incidence of AIDS-defining illnesses in the era of antiretroviral combination therapy. AIDS. 1997;11:1731–8. - PubMed
-
- Detels R, Munoz A, McFarlane G, Kingsley LA, Margolick JB, et al. Effectiveness of potent antiretroviral therapy on time to AIDS and death in men with known HIV infection duration. Multicenter AIDS Cohort Study Investigators. JAMA. 1998;280:1497–503. - PubMed
-
- Egger M, May M, Chene G, Phillips AN, Ledergerber B, et al. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies. Lancet. 2002;360:119–29. - PubMed
-
- Hogg RS, Yip B, Chan KJ, Wood E, Craib KJ, et al. Rates of disease progression by baseline CD4 cell count and viral load after initiating triple-drug therapy. JAMA. 2001;286:2568–77. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
