

Copy number variants in patients with severe oligozoospermia and Sertoli-cell-only syndrome
- PMID: 21559371
- PMCID: PMC3084853
- DOI: 10.1371/journal.pone.0019426
Copy number variants in patients with severe oligozoospermia and Sertoli-cell-only syndrome
Abstract
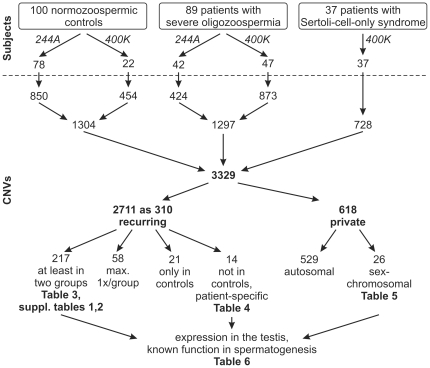
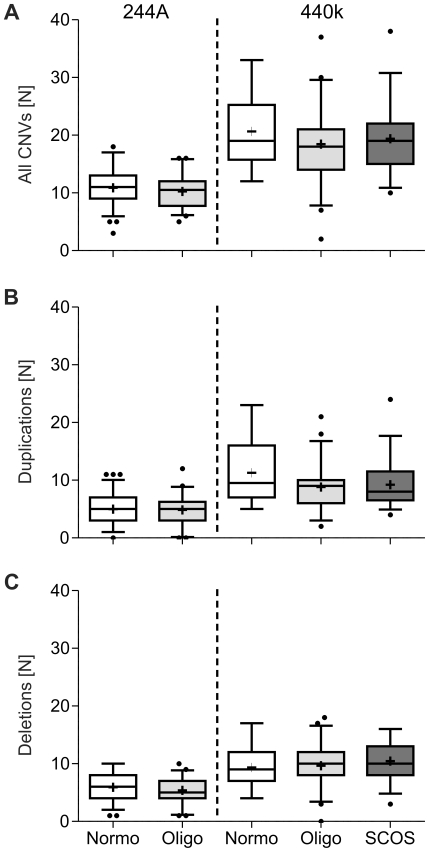
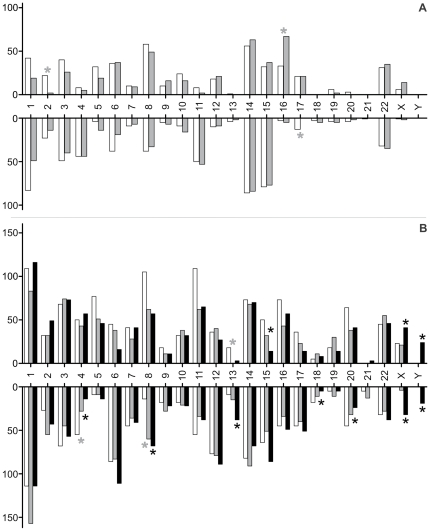
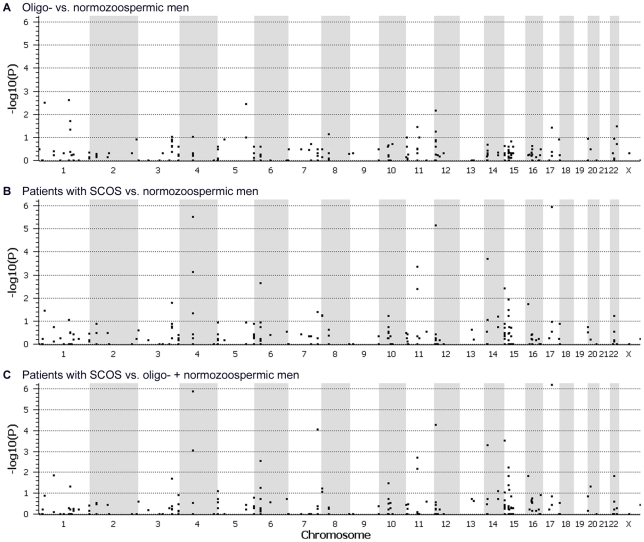
A genetic origin is estimated in 30% of infertile men with the common phenotypes of oligo- or azoospermia, but the pathogenesis of spermatogenic failure remains frequently obscure. To determine the involvement of Copy Number Variants (CNVs) in the origin of male infertility, patients with idiopathic severe oligozoospermia (N = 89), Sertoli-cell-only syndrome (SCOS, N = 37)) and controls with normozoospermia (N = 100) were analysed by array-CGH using the 244A/400K array sets (Agilent Technologies). The mean number of CNVs and the amount of DNA gain/loss were comparable between all groups. Ten recurring CNVs were only found in patients with severe oligozoospermia, three only in SCOS and one CNV in both groups with spermatogenic failure but not in normozoospermic men. Sex-chromosomal, mostly private CNVs were significantly overrepresented in patients with SCOS. CNVs found several times in all groups were analysed in a case-control design and four additional candidate genes and two regions without known genes were associated with SCOS (P<1×10(-3)). In conclusion, by applying array-CGH to study male infertility for the first time, we provide a number of candidate genes possibly causing or being risk factors for the men's spermatogenic failure. The recurring, patient-specific and private, sex-chromosomal CNVs as well as those associated with SCOS are candidates for further, larger case-control and re-sequencing studies.
Conflict of interest statement
Figures
Comment in
-
Re: Copy number variants in patients with severe oligozoospermia and sertoli-cell-only syndrome.J Urol. 2012 Jan;187(1):243-4. doi: 10.1016/j.juro.2011.09.114. Epub 2011 Nov 25. J Urol. 2012. PMID: 22153466 No abstract available.
References
-
- Tüttelmann F, Nieschlag E. Classification of andrological disorders. In: Nieschlag E, Behre HM, Nieschlag S, editors. Andrology: Male Reproductive Health and Dysfunction. Heidelberg: Springer; 2010. pp. 87–92.
-
- Tüttelmann F, Werny F, Cooper TG, Kliesch S, Simoni M, et al. Clinical experience with azoospermia: Aetiology and chances for spermatozoa detection upon biopsy. Int J Androl Jun. 2010;28 [Epub ahead of print] - PubMed
-
- Huang WJ, Yen PH. Genetics of spermatogenic failure. Sex Dev. 2008;2:251–259. - PubMed
-
- McLachlan RI, O'Bryan MK. State of the art for genetic testing of infertile men. J Clin Endocrinol Metab. 2010;95:1013–1024. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
