

Improving the characterization of radiologically isolated syndrome suggestive of multiple sclerosis
- PMID: 21559385
- PMCID: PMC3084867
- DOI: 10.1371/journal.pone.0019452
Improving the characterization of radiologically isolated syndrome suggestive of multiple sclerosis
Abstract
Objective: To improve the characterization of asymptomatic subjects with brain magnetic resonance imaging (MRI) abnormalities highly suggestive of multiple sclerosis (MS), a condition named as "radiologically isolated syndrome" (RIS).
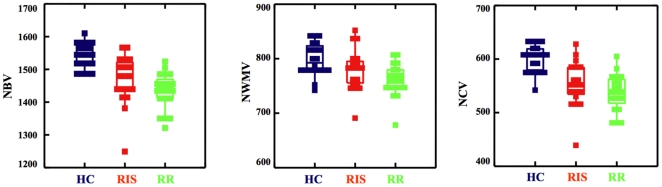
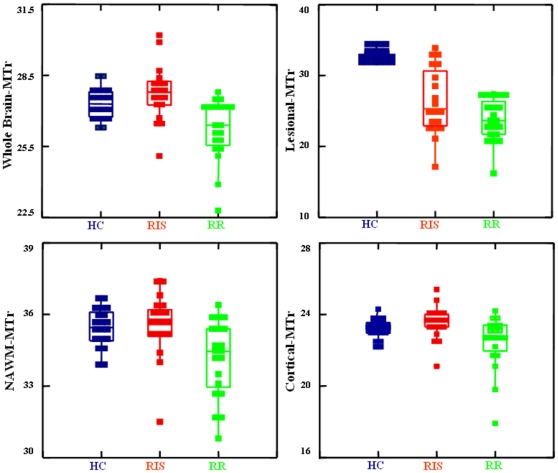
Methods: Quantitative MRI metrics such as brain volumes and magnetization transfer (MT) were assessed in 19 subjects previously classified as RIS, 20 demographically-matched relapsing-remitting MS (RRMS) patients and 20 healthy controls (HC). Specific measures were: white matter (WM) lesion volumes (LV), total and regional brain volumes, and MT ratio (MTr) in lesions, normal-appearing WM (NAWM) and cortex.
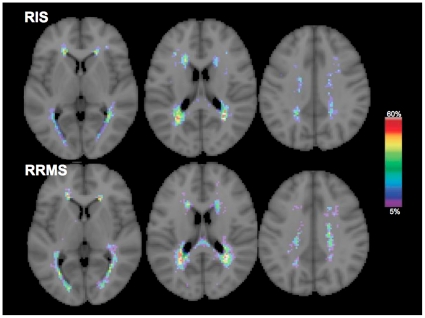
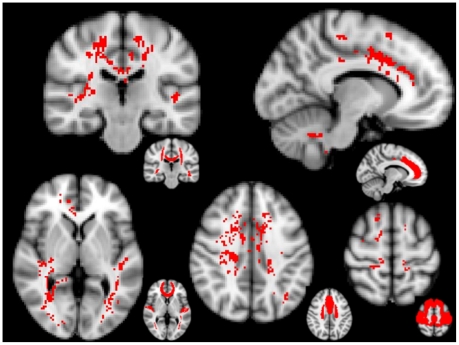
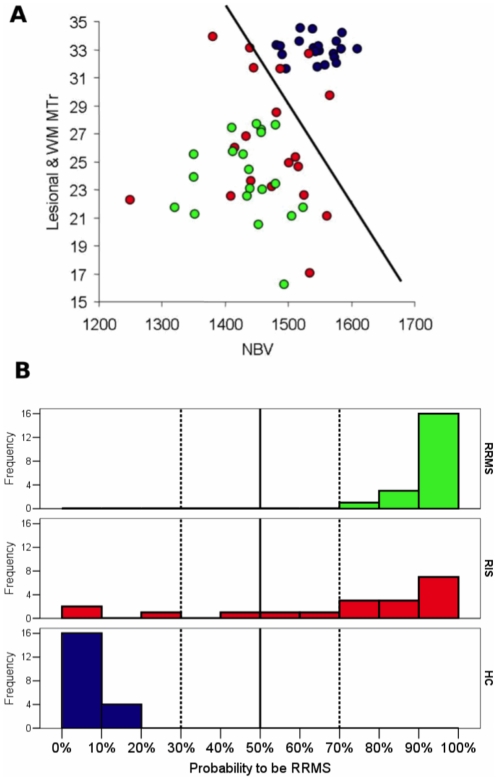
Results: LV was similar in RIS and RRMS, without differences in distribution and frequency at lesion mapping. Brain volumes were similarly lower in RRMS and RIS than in HC (p<0.001). Lesional-MTr was lower in RRMS than in RIS (p = 0.048); NAWM-MTr and cortical-MTr were similar in RIS and HC and lower (p<0.01) in RRMS. These values were particularly lower in RRMS than in RIS in the sensorimotor and memory networks. A multivariate logistic regression analysis showed that 13/19 RIS had ≥70% probability of being classified as RRMS on the basis of their brain volume and lesional-MTr values.
Conclusions: Macroscopic brain damage was similar in RIS and RRMS. However, the subtle tissue damage detected by MTr was milder in RIS than in RRMS in clinically relevant brain regions, suggesting an explanation for the lack of clinical manifestations of subjects with RIS. This new approach could be useful for narrowing down the RIS individuals with a high risk of progression to MS.
Conflict of interest statement
Figures
References
-
- Sellner J, Schirmer L, Hemmer B, Muhlau M. J Neurol; 2010. The radiologically isolated syndrome: take action when the unexpected is uncovered? - PubMed
-
- Lebrun C, Bensa C, Debouverie M, Wiertlevski S, Brassat D, et al. Association between clinical conversion to multiple sclerosis in radiologically isolated syndrome and magnetic resonance imaging, cerebrospinal fluid, and visual evoked potential: follow-up of 70 patients. Arch Neurol. 2009;66:841–846. - PubMed
-
- Siva A, Saip S, Altintas A, Jacob A, Keegan BM, et al. Multiple sclerosis risk in radiologically uncovered asymptomatic possible inflammatory-demyelinating disease. Mult Scler. 2009;15:918–927. - PubMed
-
- Okuda DT, Mowry EM, Beheshtian A, Waubant E, Baranzini SE, et al. Incidental MRI anomalies suggestive of multiple sclerosis: the radiologically isolated syndrome. Neurology. 2009;72:800–805. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
