

Complex interaction of sensory and motor signs and symptoms in chronic CRPS
- PMID: 21559525
- PMCID: PMC3084711
- DOI: 10.1371/journal.pone.0018775
Complex interaction of sensory and motor signs and symptoms in chronic CRPS
Abstract
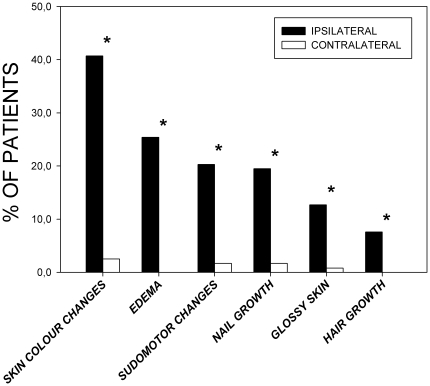
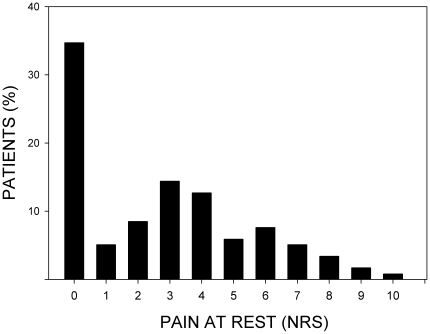
Spontaneous pain, hyperalgesia as well as sensory abnormalities, autonomic, trophic, and motor disturbances are key features of Complex Regional Pain Syndrome (CRPS). This study was conceived to comprehensively characterize the interaction of these symptoms in 118 patients with chronic upper limb CRPS (duration of disease: 43±23 months). Disease-related stress, depression, and the degree of accompanying motor disability were likewise assessed. Stress and depression were measured by Posttraumatic Stress Symptoms Score and Center for Epidemiological Studies Depression Test. Motor disability of the affected hand was determined by Sequential Occupational Dexterity Assessment and Michigan Hand Questionnaire. Sensory changes were assessed by Quantitative Sensory Testing according to the standards of the German Research Network on Neuropathic Pain. Almost two-thirds of all patients exhibited spontaneous pain at rest. Hand force as well as hand motor function were found to be substantially impaired. Results of Quantitative Sensory Testing revealed a distinct pattern of generalized bilateral sensory loss and hyperalgesia, most prominently to blunt pressure. Patients reported substantial motor complaints confirmed by the objective motor disability testings. Interestingly, patients displayed clinically relevant levels of stress and depression. We conclude that chronic CRPS is characterized by a combination of ongoing pain, pain-related disability, stress and depression, potentially triggered by peripheral nerve/tissue damage and ensuing sensory loss. In order to consolidate the different dimensions of disturbances in chronic CRPS, we developed a model based on interaction analysis suggesting a complex hierarchical interaction of peripheral (injury/sensory loss) and central factors (pain/disability/stress/depression) predicting motor dysfunction and hyperalgesia.
Conflict of interest statement
Figures






References
-
- Stanton-Hicks M, Janig W, Hassenbusch S, Haddox JD, Boas R, et al. Reflex sympathetic dystrophy: changing concepts and taxonomy. Pain. 1995;63:127–133. - PubMed
-
- Bruehl S, Harden RN, Galer BS, Saltz S, Bertram M, et al. External validation of IASP diagnostic criteria for Complex Regional Pain Syndrome and proposed research diagnostic criteria. International Association for the Study of Pain. Pain. 1999;81:147–154. - PubMed
-
- Vaneker M, Wilder-Smith OHG, Schrombges P, Oerlemans HM. Impairments as measured by ISS do not greatly change between one and eight years after CRPS 1 diagnosis. European Journal of Pain. 2006;10:639–644. - PubMed
-
- Birklein F, Kunzel W, Sieweke N. Despite clinical similarities there are significant differences between acute limb trauma and complex regional pain syndrome I (CRPS I). Pain. 2001;93:165–171. - PubMed
-
- Oaklander AL, Fields HL. Is reflex sympathetic dystrophy/complex regional pain syndrome type I a small-fiber neuropathy? Ann Neurol. 2009;65:629–638. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
