

Effects of non-steroidal anti-inflammatory drug treatments on cognitive decline vary by phase of pre-clinical Alzheimer disease: findings from the randomized controlled Alzheimer's Disease Anti-inflammatory Prevention Trial
- PMID: 21560159
- PMCID: PMC3208130
- DOI: 10.1002/gps.2723
Effects of non-steroidal anti-inflammatory drug treatments on cognitive decline vary by phase of pre-clinical Alzheimer disease: findings from the randomized controlled Alzheimer's Disease Anti-inflammatory Prevention Trial
Abstract
Objective: We examined the effects of non-steroidal anti-inflammatory drugs on cognitive decline as a function of phase of pre-clinical Alzheimer disease.
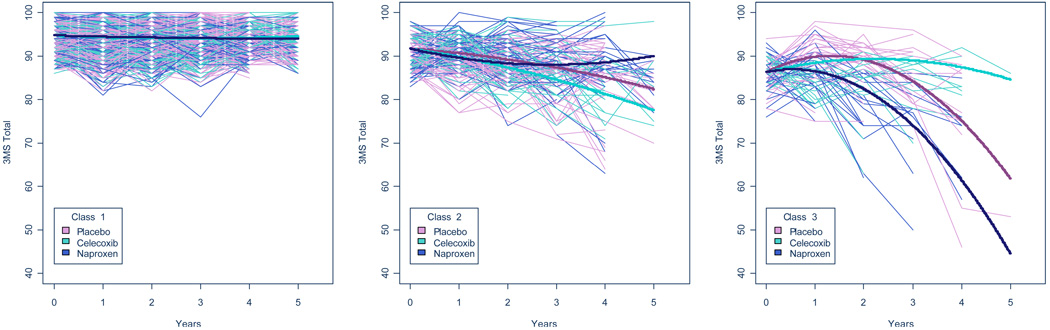
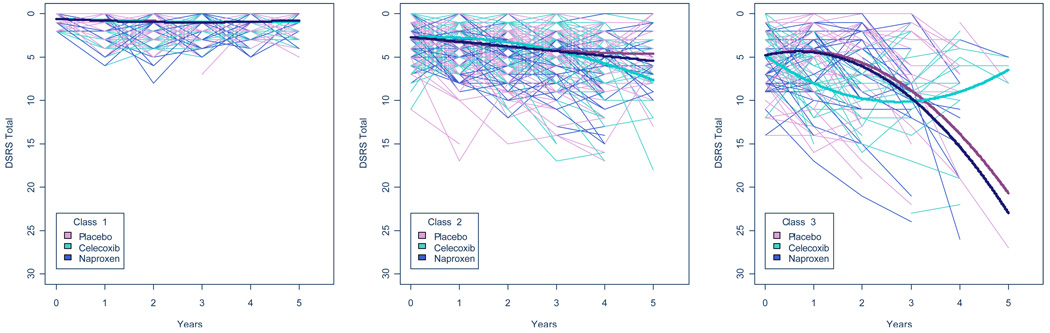
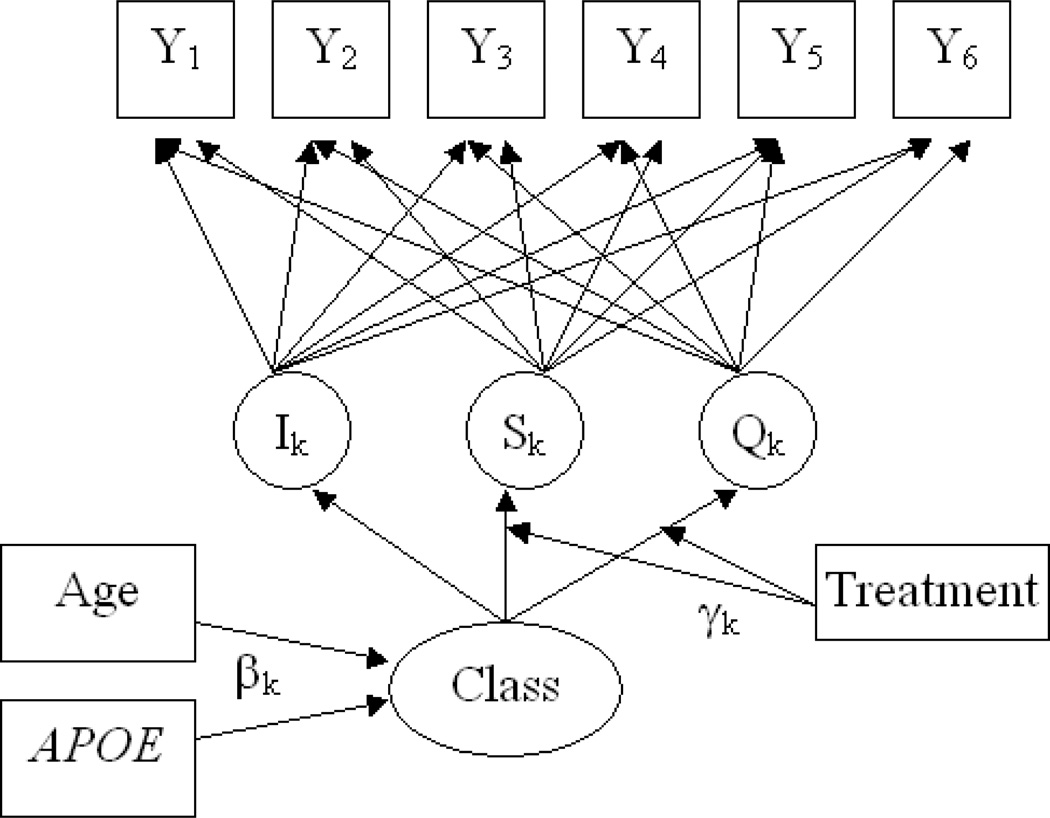
Methods: Given recent findings that cognitive decline accelerates as clinical diagnosis is approached, we used rate of decline as a proxy for phase of pre-clinical Alzheimer disease. We fit growth mixture models of Modified Mini-Mental State (3MS) Examination trajectories with data from 2388 participants in the Alzheimer's Disease Anti-inflammatory Prevention Trial and included class-specific effects of naproxen and celecoxib.
Results: We identified three classes: "no decline", "slow decline", and "fast decline", and examined the effects of celecoxib and naproxen on linear slope and rate of change by class. Inclusion of quadratic terms improved fit of the model (-2 log likelihood difference: 369.23; p < 0.001) but resulted in reversal of effects over time. Over 4 years, participants in the slow-decline class on placebo typically lost 6.6 3MS points, whereas those on naproxen lost 3.1 points (p-value for difference: 0.19). Participants in the fast-decline class on placebo typically lost 11.2 points, but those on celecoxib first declined and then gained points (p-value for difference from placebo: 0.04), whereas those on naproxen showed a typical decline of 24.9 points (p-value for difference from placebo: <0.0001).
Conclusions: Our results appeared statistically robust but provided some unexpected contrasts in effects of different treatments at different times. Naproxen may attenuate cognitive decline in slow decliners while accelerating decline in fast decliners. Celecoxib appeared to have similar effects at first but then attenuated change in fast decliners.
Copyright © 2011 John Wiley & Sons, Ltd.
Conflict of interest statement
Conflicts of Interest:
Dr. Leoutsakos has no conflicts of interest.
Dr. Muthen is a developer and owner of MPLUS, the software used for the analyses in this paper.
Dr. Breitner previously held partial royalty interests in 2 United States patents for the use of NSAIDs for the prevention of AD; in January 2005 he assigned these interests irrevocably as a gift to a private charitable foundation in which he has no constructive or beneficial interest.
Dr. Lyketsos is a consultant to GlaxoSmithKline and receives lecture honoraria and support for continuing medical education activities from AstraZeneca, Eisai, Forest Laboratories, Janssen, Lilly, Novartis, and Pfizer.
Pfizer provided celecoxib and matching placebo and Bayer Healthcare provided naproxen sodium and matching placebo for the ADAPT trial.
Figures
References
-
- AD2000 Collaborative Group. Bentham P, Gray R, Sellwood E, Hills R, Crome P, Raftery J. Aspirin in Alzheimer's disease (AD2000): a randomised open-label trial. Lancet Neurol. 2008;7(1):41–49. - PubMed
-
- ADAPT Research Group. Lyketsos CG, Breitner JC, et al. Naproxen and celecoxib do not prevent AD in early results from a randomized controlled trial. Neurology. 2007;68(21):1800–1808. - PubMed
-
- Aisen PS, Schmeidler J, Pasinetti GM. Randomized pilot study of nimesulide treatment in Alzheimer's disease. Neurology. 2002;58(7):1050–1054. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
