

Review
doi: 10.1056/NEJMra0904569.
The tumor lysis syndrome
Affiliations
- PMID: 21561350
- PMCID: PMC3437249
- DOI: 10.1056/NEJMra0904569
Item in Clipboard
Review
The tumor lysis syndrome
N Engl J Med.
.
Erratum in
-
The Tumor Lysis Syndrome.N Engl J Med. 2018 Sep 13;379(11):1094. N Engl J Med. 2018. PMID: 30209934 No abstract available.
No abstract available
Figures

The graduated cylinders shown in Panel A contain leukemic cells removed by leukapheresis from a patient with T-cell acute lymphoblastic leukemia and hyperleukocytosis (white-cell count, 365,000 per cubic millimeter). Each cylinder contains straw-colored clear plasma at the top, a thick layer of white leukemic cells in the middle, and a thin layer of red cells at the bottom. The highly cellular nature of Burkitt’s lymphoma is evident in Panel B (Burkitt’s lymphoma of the appendix, hematoxylin and eosin). Lysis of cancer cells (Panel C) releases DNA, phosphate, potassium, and cytokines. DNA released from the lysed cells is metabolized into adenosine and guanosine, both of which are converted into xanthine. Xanthine is then oxidized by xanthine oxidase, leading to the production of uric acid, which is excreted by the kidneys. When the accumulation of phosphate, potassium, xanthine, or uric acid is more rapid than excretion, the tumor lysis syndrome develops. Cytokines cause hypotension, inflammation, and acute kidney injury, which increase the risk for the tumor lysis syndrome. The bidirectional dashed line between acute kidney injury and tumor lysis syndrome indicates that acute kidney injury increases the risk of the tumor lysis syndrome by reducing the ability of the kidneys to excrete uric acid, xanthine, phosphate, and potassium. By the same token, development of the tumor lysis syndrome can cause acute kidney injury by renal precipitation of uric acid, xanthine, and calcium phosphate crystals and by crystal-independent mechanisms. Allopurinol inhibits xanthine oxidase (Panel D) and prevents the conversion of hypoxanthine and xanthine into uric acid but does not remove existing uric acid. In contrast, rasburicase removes uric acid by enzymatically degrading it into allantoin, a highly soluble product that has no known adverse effects on health.
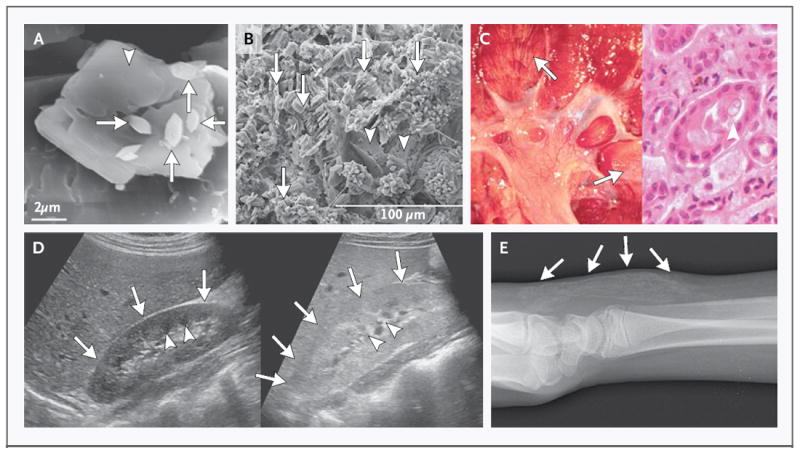
Crystallization of uric acid and calcium phosphate are the primary means of renal damage in the tumor lysis syndrome. The presence of crystals of one solute can promote crystallization of the other solutes. A scanning electron micrograph (Panel A) shows large uric acid crystals (arrowhead), which served as seeds for the formation of calcium oxalate crystals (arrows). Reprinted from Bouropoulos et al. with the permission of the publisher. In Panel B, a scanning electron micrograph shows numerous small calcium oxalate crystals (arrows) formed on larger uric acid crystals (arrowheads). Reprinted from Grases et al. with the permission of the publisher. The kidney shown in Panel C was examined at the autopsy of a 4-year-old boy who had high-grade non-Hodgkin’s lymphoma and died of acute tumor lysis syndrome. Linear yellow streaks of precipitated uric acid in the renal medulla are shown in the left panel (arrows); a single tubule containing a uric acid crystal (arrowhead) is shown in the right panel. Reprinted from Howard et al. with the permission of the publisher. In Panel D, in the normal kidney on the left, the medullary pyramids are visible deep in the kidney (arrowheads) and are surrounded by the renal cortex (arrows), which is darker than the collecting system and adjacent liver. The ultrasonographic image on the right shows a kidney from a patient with the tumor lysis syndrome, in which there is loss of the normal corticomedullary differentiation (arrowheads) and poor visualization of the renal pyramids. The brightness is similar to that of the adjacent liver (arrows), and the kidney is abnormally enlarged. Soft-tissue calcification of the dorsum of the distal forearm (Panel E) occurred in a 15-year-old boy with acute lymphoblastic leukemia and an initial white-cell count of 283,000 per cubic millimeter in whom tumor lysis syndrome, hyperphosphatemia, and symptomatic hypocalcemia developed. Several weeks after the treatment of hypocalcemia with multiple doses of intravenous calcium carbonate administered by means of a peripheral intravenous catheter in the dorsum of the hand, ectopic calcification was confirmed radiographically (arrows). Reprinted from Howard et al. with the permission of the publisher.

This algorithm presents a guide to care at the time of patient presentation. Subsequent care depends on how the patient progresses. The tumor lysis syndrome unexpectedly develops in some patients who are at low risk, and they require more aggressive treatment, and some high-risk patients have no evidence of the tumor lysis syndrome after a few days of treatment and need less intensive care after the initial period. Assessment of risk factors for the tumor lysis syndrome requires clinical judgment. It may not always be clear whether mild or transient dehydration should count, whether a cancer mass is medium or large, or whether the potential for cell lysis of a particular cancer with a particular treatment is medium or high. In equivocal cases, other criteria can be useful to clarify the degree of risk: an elevated lactate dehydrogenase level (>2 times the upper limit of the normal range) and an elevated uric acid level at presentation are associated with an increased risk of the tumor lysis syndrome and can be used to help classify borderline cases into a suitable risk group. If it is difficult to distinguish between two categories, treat the patient as if he or she is in the higher-risk category. Because the algorithm presented is designed for use by both oncologists and non-oncologists, a conservative approach is presented to maximize safety. “Bulky tumor” includes the tumor mass from metastatic lesions. TLS denotes tumor lysis syndrome.
Comment in
-
The tumor lysis syndrome.N Engl J Med. 2011 Aug 11;365(6):573; author reply 573-4. doi: 10.1056/NEJMc1106641. N Engl J Med. 2011. PMID: 21830980 No abstract available.
-
The tumor lysis syndrome.N Engl J Med. 2011 Aug 11;365(6):572-3; author reply 573-4. doi: 10.1056/NEJMc1106641. N Engl J Med. 2011. PMID: 21830981 No abstract available.
-
The tumor lysis syndrome.N Engl J Med. 2011 Aug 11;365(6):571-2; author reply 573-4. doi: 10.1056/NEJMc1106641. N Engl J Med. 2011. PMID: 21830982 Free PMC article. No abstract available.
References
-
- Abu-Alfa AK, Younes A. Tumor lysis syndrome and acute kidney injury: evaluation, prevention, and management. Am J Kidney Dis. 2010;55(Suppl 3):S1–S13. - PubMed
-
- Cairo MS, Coiffier B, Reiter A, Younes A. Recommendations for the evaluation of risk and prophylaxis of tumour lysis syndrome (TLS) in adults and children with malignant diseases: an expert TLS panel consensus. Br J Haematol. 2010;149:578–86. - PubMed
-
- Gertz MA. Managing tumor lysis syndrome in 2010. Leuk Lymphoma. 2010;51:179–80. - PubMed
-
- Magrath IT, Semawere C, Nkwocha J. Causes of death in patients with Burkitt’s lymphoma — the role of supportive care in overall management. East Afr Med J. 1974;51:623–32. - PubMed
-
- Krishnan G, D’Silva K, Al-Janadi A. Cetuximab-related tumor lysis syndrome in metastatic colon carcinoma. J Clin Oncol. 2008;26:2406–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical