

Proton pump inhibitor use and risk of adverse cardiovascular events in aspirin treated patients with first time myocardial infarction: nationwide propensity score matched study
- PMID: 21562004
- PMCID: PMC3092520
- DOI: 10.1136/bmj.d2690
Proton pump inhibitor use and risk of adverse cardiovascular events in aspirin treated patients with first time myocardial infarction: nationwide propensity score matched study
Abstract
Objective: To examine the effect of proton pump inhibitors on adverse cardiovascular events in aspirin treated patients with first time myocardial infarction.
Design: Retrospective nationwide propensity score matched study based on administrative data. Setting All hospitals in Denmark.
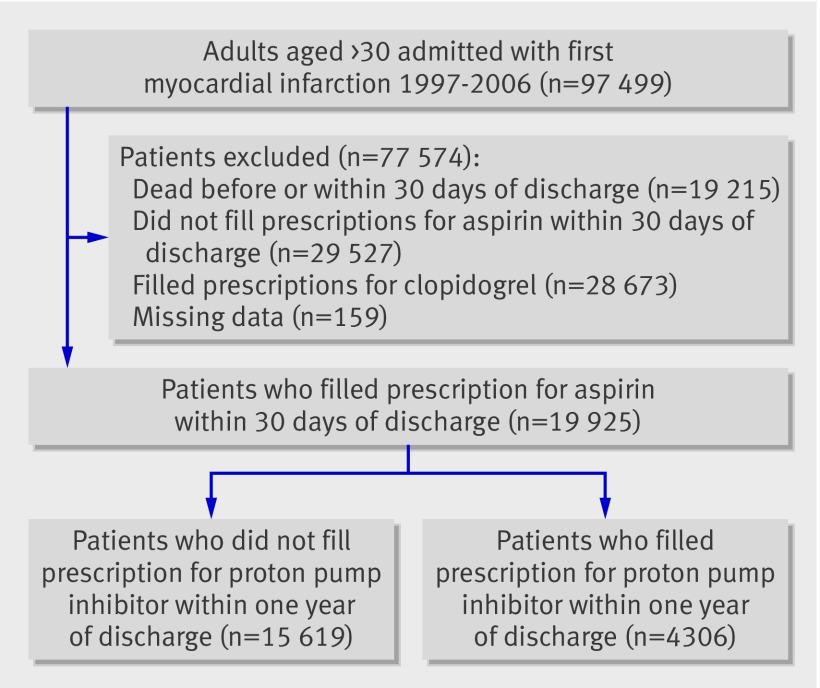
Participants: All aspirin treated patients surviving 30 days after a first myocardial infarction from 1997 to 2006, with follow-up for one year. Patients treated with clopidogrel were excluded.
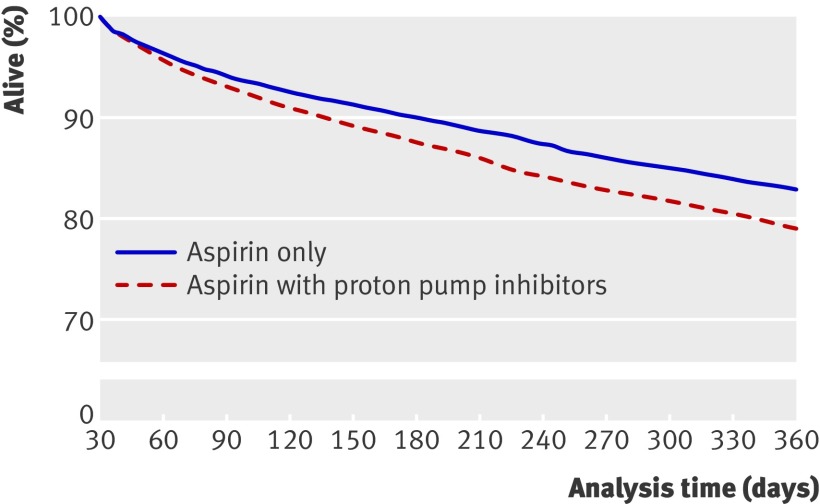
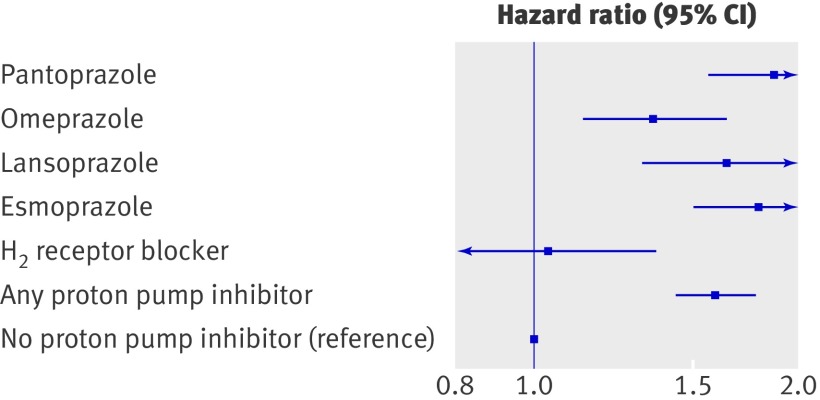
Main outcome measures: The risk of the combined end point of cardiovascular death, myocardial infarction, or stroke associated with use of proton pump inhibitors was analysed using Kaplan-Meier analysis, Cox proportional hazard models, and propensity score matched Cox proportional hazard models. Results 3366 of 19,925 (16.9%) aspirin treated patients experienced recurrent myocardial infarction, stroke, or cardiovascular death. The hazard ratio for the combined end point in patients receiving proton pump inhibitors based on the time dependent Cox proportional hazard model was 1.46 (1.33 to 1.61; P<0.001) and for the propensity score matched model based on 8318 patients it was 1.61 (1.45 to 1.79; P<0.001). A sensitivity analysis showed no increase in risk related to use of H(2) receptor blockers (1.04, 0.79 to 1.38; P=0.78). Conclusion In aspirin treated patients with first time myocardial infarction, treatment with proton pump inhibitors was associated with an increased risk of adverse cardiovascular events.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures

Comment in
-
Patients treated with aspirin after a first myocardial infarction who also receive a proton pump inhibitor have a higher incidence of cardiovascular events.Evid Based Med. 2012 Feb;17(1):33-4. doi: 10.1136/ebmed.2011.100263. Epub 2011 Nov 22. Evid Based Med. 2012. PMID: 22108076 No abstract available.
References
-
- Smith SC Jr, Allen J, Blair SN, Bonow RO, Brass LM, Fonarow GC, et al. AHA/ACC guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease: 2006 update: endorsed by the National Heart, Lung, and Blood Institute. Circulation 2006;113:2363-72. - PubMed
-
- Bhatt DL, Scheiman J, Abraham NS, Antman EM, Chan FK, Furberg CD, et al. ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents. Circulation 2008;118:1894-909. - PubMed
-
- Giraud MN, Sanduja SK, Felder TB, Illich PA, Dial EJ, Lichtenberger LM. Effect of omeprazole on the bioavailability of unmodified and phospholipid-complexed aspirin in rats. Aliment Pharmacol Ther 1997;11:899-906. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical