

Assessment of variation in live donor kidney transplantation across transplant centers in the United States
- PMID: 21562451
- PMCID: PMC3462439
- DOI: 10.1097/TP.0b013e31821bf138
Assessment of variation in live donor kidney transplantation across transplant centers in the United States
Abstract
Background: Transplant centers vary in the proportion of kidney transplants performed using live donors. Clinical innovations that facilitate live donation may drive this variation.
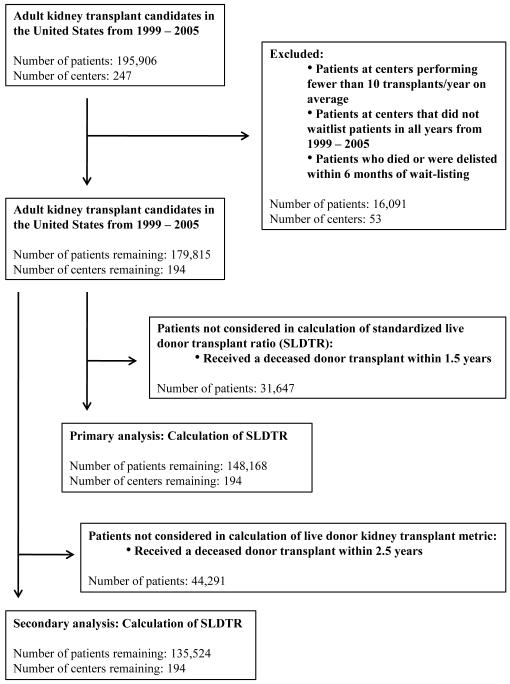
Methods: We assembled a cohort of renal transplant candidates at 194 US centers using registry data from 1999 to 2005. We measured magnitude of live donor kidney transplantation (LDKTx) through development of a standardized live donor transplantation ratio (SLDTR) at each center that accounted for center population differences. We examined associations between center characteristics and the likelihood that individual transplant candidates underwent LDKTx. To identify practices through which centers increase LDKTx, we also examined center characteristics associated with consistently being in the upper three quartiles of SLDTR.
Results: The cohort comprised 148,168 patients, among whom 34,593 (23.3%) underwent LDKTx. In multivariable logistic regression, candidates had an increased likelihood of undergoing LDKTx at centers with greater use of "unrelated donors" (defined as nonspouses and nonfirst-degree family members of the recipient; odds ratio [OR] 1.31 for highest vs. lowest use; P=0.02) and at centers with programs to overcome donor-recipient incompatibility (OR 1.33; P=0.01). Centers consistently in the upper three SLDTR quartiles were also more likely to use "unrelated" donors (OR 8.30 per tertile of higher use; P<0.01), to have incompatibility programs (OR 4.79, P<0.01), and to use laparoscopic nephrectomy (OR 2.53 per tertile of higher use; P=0.02).
Conclusion: Differences in center population do not fully account for differences in the use of LDKTx. To maximize opportunities for LDKTx, centers may accept more unrelated donors and adopt programs to overcome biological incompatibility.
References
-
- Davis CL, Delmonico FL. Living-donor kidney transplantation: a review of the current practices for the live donor. J Am Soc Nephrol. 2005;16(7):2098. - PubMed
-
- Kasiske BL, Snyder JJ, Matas AJ, Ellison MD, Gill JS, Kausz AT. Preemptive kidney transplantation: the advantage and the advantaged. J Am Soc Nephrol. 2002;13(5):1358. - PubMed
-
- Lawthers AG, McCarthy EP, Davis RB, Peterson LE, Palmer RH, Iezzoni LI. Identification of in-hospital complications from claims data. Is it valid? Med Care. 2000;38(8):785. - PubMed
-
- Segev DL, Gentry SE, Warren DS, Reeb B, Montgomery RA. Kidney paired donation and optimizing the use of live donor organs. JAMA. 2005;293(15):1883. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
