

Interventions for trichomoniasis in pregnancy
- PMID: 21563127
- PMCID: PMC7044808
- DOI: 10.1002/14651858.CD000220.pub2
Interventions for trichomoniasis in pregnancy
Abstract
Background: Vaginitis due to Trichomonas vaginalis is one of the most common of sexually transmitted diseases. Trichomoniasis affects women during pregnancy as well but it is not clearly established whether it causes preterm birth and other pregnancy complications.
Objectives: The objective of this review was to assess the effects of various treatments for trichomoniasis during pregnancy.
Search strategy: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (14 January 2011).
Selection criteria: Randomized trials comparing anti-trichomonas agents during pregnancy. Trials including symptomatic or asymptomatic women with trichomoniasis were eligible.
Data collection and analysis: Two review authors assessed eligibility and trial quality.
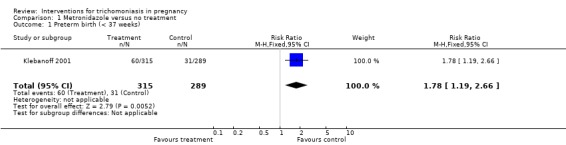
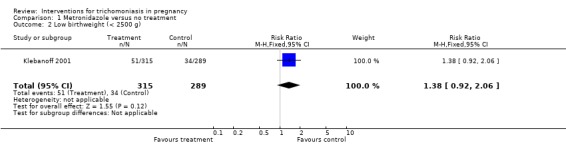
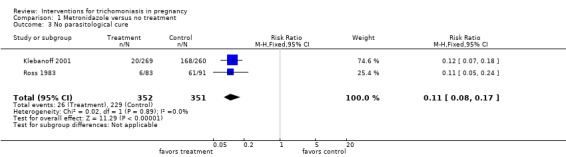
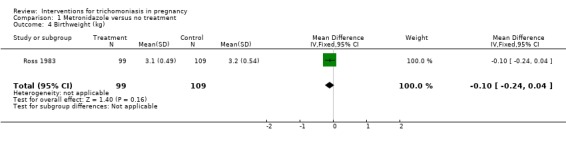
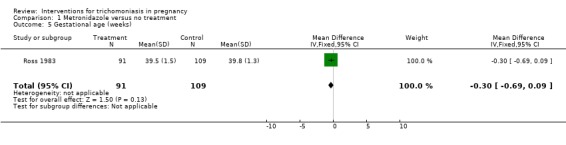
Main results: We included two trials with 842 pregnant women. In both trials around 90% of women were cleared of trichomonas in the vagina after treatment. In the US trial, women with asymptomatic trichomoniasis between 16 and 23 weeks were treated with metronidazole on two occasions at least two weeks apart. The trial was stopped before reaching its target recruitment because metronidazole was not effective in reducing preterm birth and there was a likelihood of harm (risk ratio 1.78; 95% confidence interval 1.19 to 2.66). The South African trial recruited women later in pregnancy and did not have the design and power to address adverse clinical outcomes. We excluded two recent studies, identified for the current update, because they did not address the primary question.
Authors' conclusions: Metronidazole, given as a single dose, is likely to provide parasitological cure for trichomoniasis, but it is not known whether this treatment will have any effect on pregnancy outcomes. The cure rate could probably be higher if more partners used the treatment.
Conflict of interest statement
None known.
Figures
Update of
-
Interventions for trichomoniasis in pregnancy.Cochrane Database Syst Rev. 2002;(3):CD000220. doi: 10.1002/14651858.CD000220. Cochrane Database Syst Rev. 2002. Update in: Cochrane Database Syst Rev. 2011 May 11;(5):CD000220. doi: 10.1002/14651858.CD000220.pub2. PMID: 12137609 Updated.
References
References to studies included in this review
Klebanoff 2001 {published data only}
-
- Carey JC, Klebanoff M for the NICHD MFMU Network. Metronidazole treatment increased the risk of preterm birth in asymptomatic women with trichomonas. American Journal of Obstetrics and Gynecology 2000;182(1):Ss13.
-
- Klebanoff M, Carey C, Hauth J, Hillier S, Nugent R, Thom E, et al. Failure of metronidazole to prevent preterm delivery among pregnant women with asymptomatic trichomonas vaginalis infection. New England Journal of Medicine 2001;345(7):487‐93. - PubMed
Ross 1983 {published data only}
-
- Ross SM, Middelkoop A. Trichomonas infection in pregnancy ‐ does it affect perinatal outcome?. South African Medical Journal 1983;63:566‐7. - PubMed
References to studies excluded from this review
Kigozi 2003 {published data only}
-
- Kigozi GG, Brahmbhatt H, Wabwire‐Mangen F, Wawer MJ, Serwadda D, Sewankambo N, et al. Treatment of trichomonas in pregnancy and adverse outcomes of pregnancy: a subanalysis of a randomized trial in Rakai, Uganda. American Journal of Obstetrics and Gynecology 2003;189:1398‐400. - PubMed
Robinson 1965 {published data only}
-
- Robinson SC, Gopi M. Trichomonas vaginalis. V. Further observations on metronidazole (Flagyl) (including infant follow‐up). American Journal of Obstetrics and Gynecology 1965;93:502‐5. - PubMed
Roos 1978 {published data only}
-
- Roos RF. Trichomoniasis treated with a single dose of benzoylmetronidazole. South African Medical Journal 1978;54:869‐70. - PubMed
Stringer 2010 {published data only}
Additional references
Clarke 2000
-
- Clarke M, Oxman AD, editors. Cochrane Reviewers’ Handbook 4.1 [updated June 2000]. In: Review Manager (RevMan) [Computer program]. Version 4.1. Oxford, England: The Cochrane Collaboration, 2000.
Cotch 1997
-
- Cotch MF, Pastorek JG 2nd, Nugent RP, Hillier SL, Gibbs RS, Martin DH, et al. Trichomonas vaginalis associated with low birth weight and preterm delivery. The Vaginal Infections and Prematurity Study Group. Sexually Transmitted Diseases 1997;24(6):353‐60. - PubMed
Forna 2003
French 1999
-
- French JI, McGregor JA, Draper D, Parker R, McFee J. Gestational bleeding, bacterial vaginosis, and common reproductive tract infections: risk for preterm birth and benefit of treatment. Obstetrics and Gynecology 1999;93:715‐24. - PubMed
Hauth 1995
-
- Hauth JC, Goldenberg RL, Andrews WW, DuBard MB, Copper RL. Reduced incidence of preterm delivery with metronidazole and erythromycin in women with bacterial vaginosis. New England Journal of Medicine 1995;333:1732‐6. - PubMed
Higgins 2008
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1 [updated September 2008]. The Cochrane Collaboration, 2008. Available from www.cochrane‐handbook.org.
Lossick 1991
-
- Lossick JG, Kent HL. Trichomoniasis: trends in diagnosis and management. American Journal of Obstetrics and Gynecology 1991;165:1217‐22. - PubMed
McDonald 1997
-
- McDonald HM, O'Loughlin JA, Vigneswaran R, Jolley PT, Harvey JA, Bof A, et al. Impact of metronidazole therapy on preterm birth in women with bacterial vaginosis flora (Gardnerella vaginalis): a randomised, placebo controlled trial. British Journal of Obstetrics and Gynaecology 1997;104(12):1391‐7. - PubMed
Morales 1994
-
- Morales WJ, Schorr S, Albritton J. Effect of metronidazole in patients with preterm birth in preceding pregnancy and bacterial vaginosis: a placebo‐controlled, double‐blind study. American Journal of Obstetrics and Gynecology 1994;171:345‐9. - PubMed
Murphy 1994
-
- Murphy PA, Jones E. Use of oral metronidazole in pregnancy. Journal of Nurse Midwifery 1994;39:214‐20. - PubMed
RevMan 2008 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.0. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2008.
Sorvillo 2001
WHO 2011
-
- World Health Organization. Prevalence and incidence of selected sexually transmitted infections. Chlamydia, Neisseria gonorrhoeae, syphilis and Trichomonas vaginalis. Geneva: WHO, in press.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical