

Support of cancer patients' spiritual needs and associations with medical care costs at the end of life
- PMID: 21563177
- PMCID: PMC3177963
- DOI: 10.1002/cncr.26221
Support of cancer patients' spiritual needs and associations with medical care costs at the end of life
Abstract
Background: Although spiritual care is associated with less aggressive medical care at the end of life (EOL), it remains infrequent. It is unclear if the omission of spiritual care impacts EOL costs.
Methods: A prospective, multisite study of 339 advanced cancer patients accrued subjects from September 2002 to August 2007 from an outpatient setting and followed them until death. Spiritual care was measured by patients' reports that the health care team supported their religious/spiritual needs. EOL costs in the last week were compared among patients reporting that their spiritual needs were inadequately supported versus those who reported that their needs were well supported. Analyses were adjusted for confounders (eg, EOL discussions).
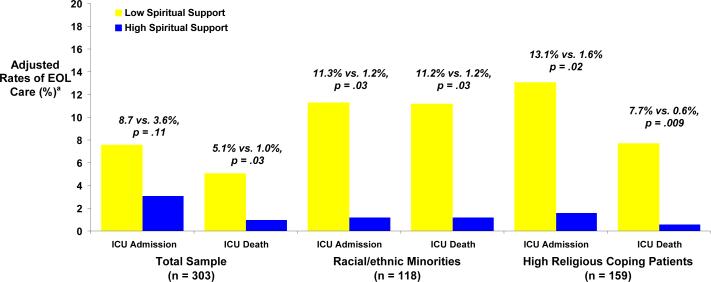
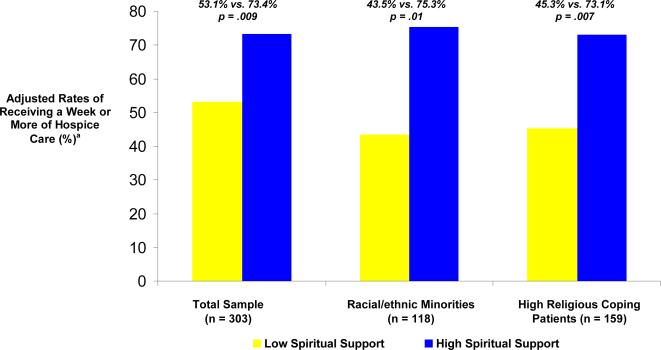
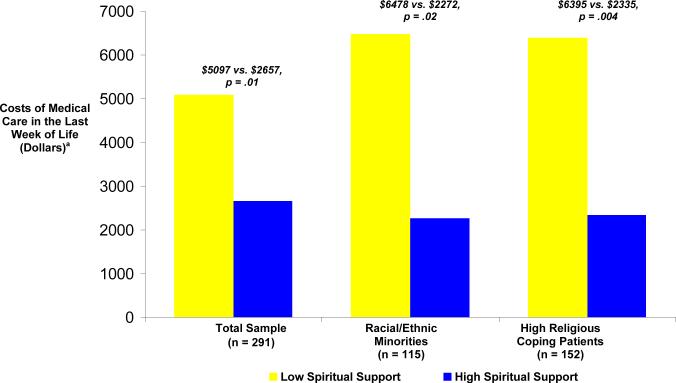
Results: Patients reporting that their religious/spiritual needs were inadequately supported by clinic staff were less likely to receive a week or more of hospice (54% vs 72.8%; P = .01) and more likely to die in an intensive care unit (ICU) (5.1% vs 1.0%, P = .03). Among minorities and high religious coping patients, those reporting poorly supported religious/spiritual needs received more ICU care (11.3% vs 1.2%, P = .03 and 13.1% vs 1.6%, P = .02, respectively), received less hospice (43.% vs 75.3% ≥1 week of hospice, P = .01 and 45.3% vs 73.1%, P = .007, respectively), and had increased ICU deaths (11.2% vs 1.2%, P = .03 and 7.7% vs 0.6%, P = .009, respectively). EOL costs were higher when patients reported that their spiritual needs were inadequately supported ($4947 vs $2833, P = .03), particularly among minorities ($6533 vs $2276, P = .02) and high religious copers ($6344 vs $2431, P = .005).
Conclusions: Cancer patients reporting that their spiritual needs are not well supported by the health care team have higher EOL costs, particularly among minorities and high religious coping patients.
Copyright © 2011 American Cancer Society.
Figures
References
-
- National Consensus Project for Quality Palliative Care: Clinical practice guidelines for quality palliative care. Second Edition. 2009. [accessed June 28, 2010]. Available from URL: http://www.nationalconsensusproject.org/
-
- Alcorn SR, Balboni MJ, Prigerson HG, et al. “If God wanted me yesterday, I wouldn't be here today”: religious and spiritual themes in patients' experiences of advanced cancer. J Palliat Med. 2010;13(5):581–8. - PubMed
-
- Hui D, de la Cruz M, Thorney S, Parsons HA, Delgado-Guay M, Bruera E. The Frequency and Correlates of Spiritual Distress Among Patients With Advanced Cancer Admitted to an Acute Palliative Care Unit. Am J Hosp Palliat Care - PubMed
-
- Moadel A, Morgan C, Fatone A, et al. Seeking meaning and hope: self-reported spiritual and existential needs among an ethnically-diverse cancer patient population. Psychooncology. 1999;8(5):378–85. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
