

Negative pressure wound therapy using gauze and foam: histological, immunohistochemical and ultrasonography morphological analysis of the granulation tissue and scar tissue. Preliminary report of a clinical study
- PMID: 21564551
- PMCID: PMC7950553
- DOI: 10.1111/j.1742-481X.2011.00798.x
Negative pressure wound therapy using gauze and foam: histological, immunohistochemical and ultrasonography morphological analysis of the granulation tissue and scar tissue. Preliminary report of a clinical study
Abstract
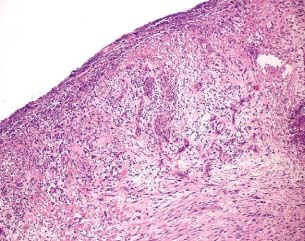
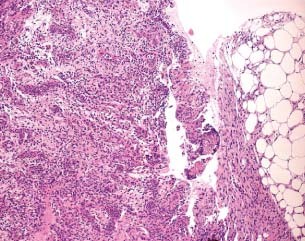
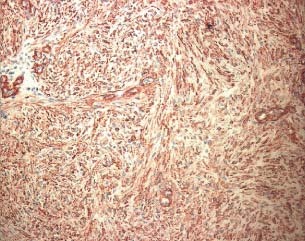
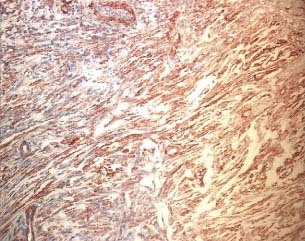
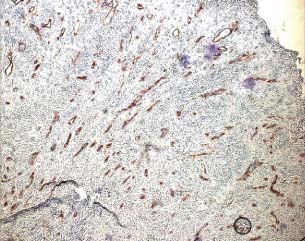
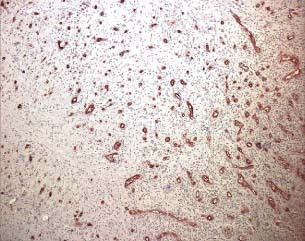
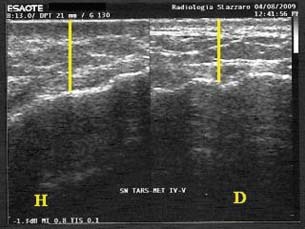
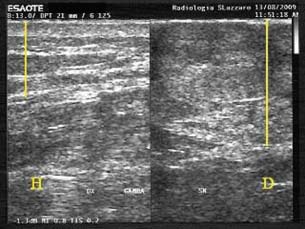
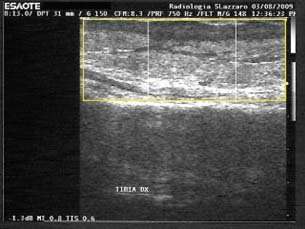
Negative pressure wound therapy (NPWT) is becoming routine for the preparation of wounds prior to grafting for wound closure. We have been using both foam- and gauze-based NPWT to prepare wounds for closure prior to skin grafting and have obtained similar proportions of closed wounds; 7/7 for wounds treated with gauze-based NPWT and 11/11 for wounds treated with foam-based NPWT. In our follow-up consultations we observed that skin grafts on the foam-treated patients were less pliable than those on the gauze-treated patients. To assess what the mechanism of this effect might be, we compared the specific details of the treatments of both 11 foam and 7 gauze patients, including depth, location, patients' age and co-morbidity; biopsies of granulation and scar tissue were taken and stained with haematoxylin-eosin and by Masson's trichrome staining and conducted ultrasound analysis of the closed wounds, to see if there were features which explained those effects. All foam patients were treated at -125 mm Hg for an average of 25·9 days before skin grafts were applied. All gauze patients were treated at -80 mm Hg for an average of 24·7 days before skin grafts were applied. Biopsies of granulation tissue prior to skin grafting from five foam and four gauze-based NPWT patients did not reveal any obvious histological differences between the treatments. Ultrasound analysis of the skin-grafted wounds showed an average depth of scar tissue of 18 mm in the wound beds of the foam-treated wounds and 7 mm in the gauze-treated ones. Biopsies taken on the scar tissue after treatment with the gauze showed a minor tissue thickness and disorganisation and less sclerotic components. The findings of this preliminary analysis suggest that foam-based NPWT may induce a thicker layer of scar tissue beneath skin grafts than gauze-based NPWT which might explain a reduced pliability of the reconstructed bed. At present it is unclear which mechanism might be responsible for the difference in pressure (-125 versus -80 mm Hg), either the length of the time taken to reconstruct the wound bed or the intrinsic nature of the foam or gauze on the tissue surface. Prospective studies are necessary to investigate whether these preliminary observations are confirmed and to investigate what the mechanism might be.
© 2011 The Authors. © 2011 Blackwell Publishing Ltd and Medicalhelplines.com Inc.
Figures

References
-
- KCI. V.A.C.: recommended guidelines for use. Physician & Caregiver Reference Manual . San Antonio, TX: KCI, 2002, 2‐B‐128.
-
- Smith&Nephew. V1STA™. Recommended using protocol., authors
-
- Argenta LC, Morykwas MJ, Marks MW, DeFranzo AJ, Molnar JA, David LR. Vacum‐assisted closure: state of clinical art. Plast Reconstr Surg 2006;117:127S–42S. - PubMed
-
- Kostiuchenok II, Kolker VA, Karlov VA. The vacuum effect in the surgical treatment of purulent wounds. Vestnik Khirurgii 1986;9:18–21. - PubMed
-
- Davydov YA, Malafeeva AP, Smirnov AP. Vacuum therapy in the treatment of purulent lactation mastitis. Vestnik Khirurgii 1986;9:66–70. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
