

Obesity is an independent risk factor for clinical decompensation in patients with cirrhosis
- PMID: 21567436
- PMCID: PMC3144991
- DOI: 10.1002/hep.24418
Obesity is an independent risk factor for clinical decompensation in patients with cirrhosis
Abstract
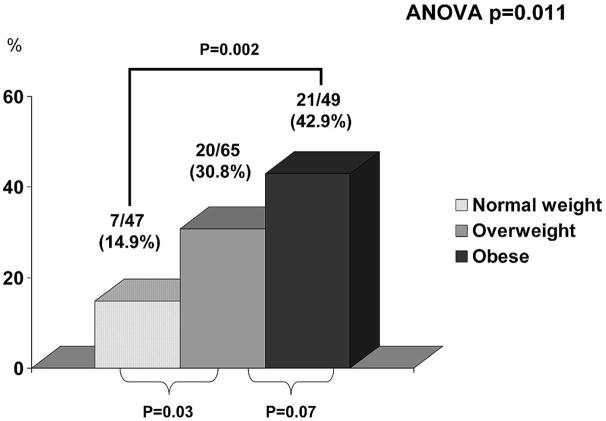
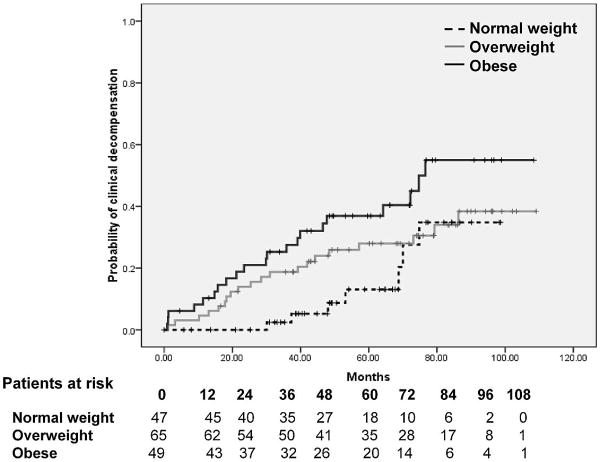
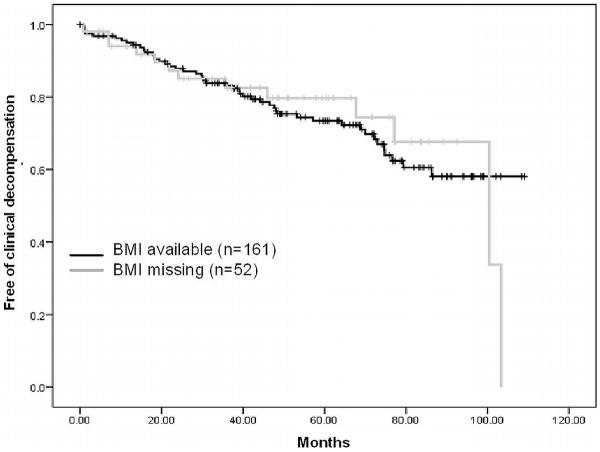
Obesity is associated with an aggressive course in chronic viral hepatitis; however, its impact in the development of clinical decompensation (CD) in patients with established cirrhosis is uncertain. We evaluated the role of obesity, in relationship to other recognized predictors, in the development of CD in patients with compensated cirrhosis. The study population, a subset of patients included in a randomized trial of beta-blockers in the prevention of varices in whom data on body mass index (BMI) was available, consisted of 161 patients with compensated cirrhosis. Laboratory tests and portal pressure (assessed by the hepatic venous pressure gradient or HVPG) were assessed on inclusion. Patients were followed until CD (ascites, hepatic encephalopathy, or variceal hemorrhage), or until September 2002. Altogether, 29% had a normal BMI, 40% were overweight, and 30% were obese. In a median follow-up of 59 months, CD occurred in 48/161 (30%) patients with an increasingly higher rate according to BMI group (15% in those with normal BMI; 31% in overweight; 43% in obese patients, P=0.011). The actuarial probability of developing CD was significantly higher in the abnormal BMI groups (P=0.022). In a multivariate model that included parameters previously identified as being predictive of CD (HVPG, albumin, Mayo endstage liver disease score), etiology, and treatment group, BMI (hazard ration 1.06; 95% confidence interval 1.01-1.12), P=0.02] was an independent predictor of decompensation, together with HVPG and albumin.
Conclusion: Obesity has a deleterious effect on the natural history of compensated cirrhosis of all etiologies, independent of portal pressure and liver function. Weight reduction may be a valuable therapeutic measure in this patient population.
Copyright © 2011 American Association for the Study of Liver Diseases.
Conflict of interest statement
No financial conflicts of interest are declared for any of the authors.
Figures
Comment in
-
To feed or what to feed in cirrhosis?Hepatology. 2012 Oct;56(4):1590. doi: 10.1002/hep.24771. Epub 2012 Jul 6. Hepatology. 2012. PMID: 22095649 No abstract available.
References
-
- D'Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol. 2006;44:217–231. - PubMed
-
- Ripoll C, Groszmann R, Garcia-Tsao G, Grace N, Burroughs A, Planas R, et al. Hepatic venous pressure gradient predicts clinical decompensation in patients with compensated cirrhosis. Gastroenterology. 2007;133:481–488. - PubMed
-
- Ogden CL, Yanovski SZ, Carroll MD, Flegal KM. The epidemiology of obesity. Gastroenterology. 2007;132:2087–2102. - PubMed
-
- World Health Organization (WHO) Report of a WHO Consultation. Geneva: World Health Organization; 2000. Obesity: preventing and managing the global epidemic. - PubMed
-
- World Health Organization. Report of a Joint FAO/WHO Expert Consultation. Geneva: World Health Organization; 2003. Diet, Nutrition and the Prevention of Chronic Diseases.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical