

Review
Hemorrhagic stroke: aneurysmal subarachnoid hemorrhage
Affiliations
- PMID: 21568235
- PMCID: PMC6189155
Item in Clipboard
Review
Hemorrhagic stroke: aneurysmal subarachnoid hemorrhage
Mo Med.
2011 Mar-Apr.
Abstract
Non-traumatic subarachnoid hemorrhage (SAH) represents approximately 5-6% of all strokes. Morbidity and mortality rates remain high, but accurate diagnosis using clinical assessment and neuroimaging, critical care management, and early treatment using either surgical or interventional techniques have improved overall outcomes. This, the fifth in a Missouri Medicine series on stroke, summarizes the clinical and imaging aspects of making the diagnosis of SAH, critical care management of the patient, treatment options, and factors important in prognosis.
Figures
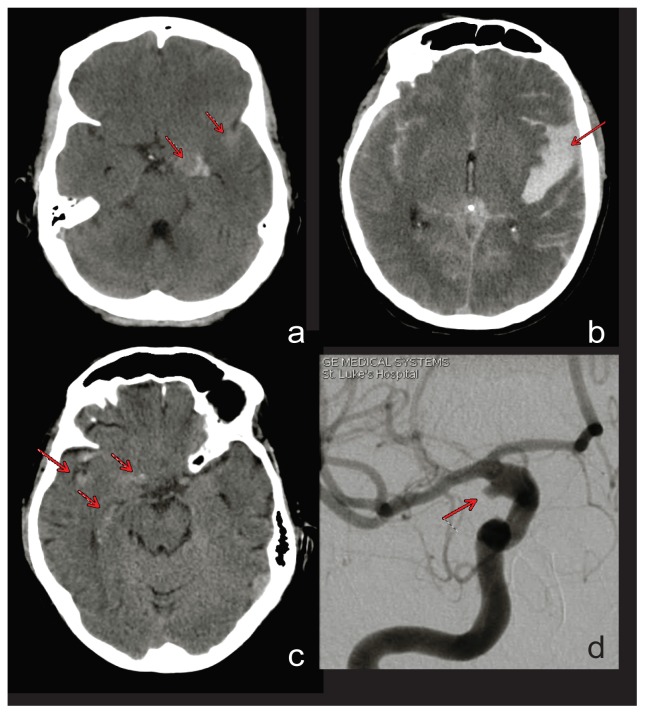
Figure 1A - Calcified giant left posterior communicating artery aneurysm (medial arrow) with associated mild subarachnoid bleeding (lateral arrow). Figure 1B - Left parasylvian hematoma and SAH resulting in right hemiparesis and aphasia due to a left middle cerebral artery aneurysm. Figure 1C - Mild subarachnoid bleeding in a patient with moderate headache and no identifiable aneurysm on CTA. Figure 1D - Digital subtraction angiography of same patient shown in 1C demonstrating a right internal carotid artery dissecting aneurysm.
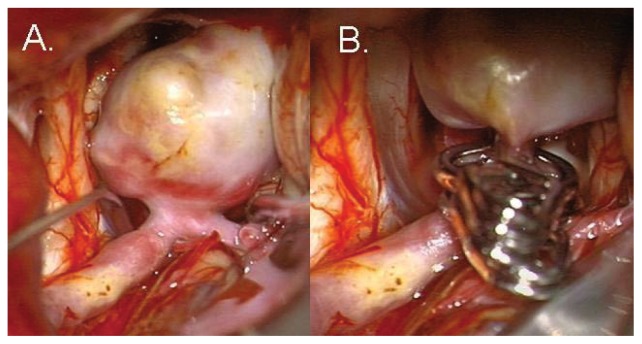
Figure 2A - Surgical visualization of the aneurysm. Figure 2B - Surgical clip in place securing the aneurysm. Photo courtesy of Michael T. Lawton, MD.
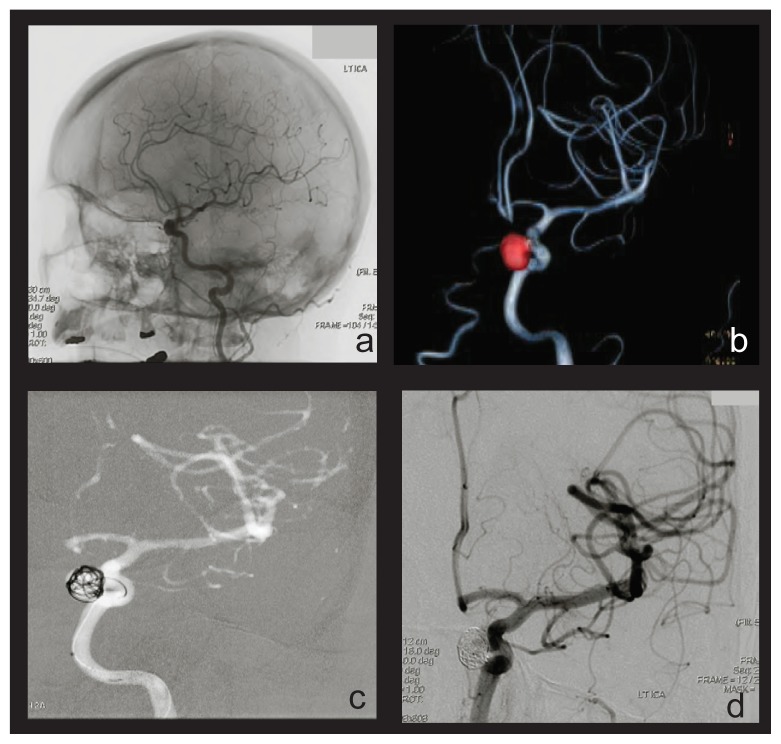
Figure 3A - Image acquisition during digital subtraction angiography. Figure 3B - Three-dimensional computer modeling of a periophthalmic aneurysm of the left internal carotid artery. The aneurysm is rendered in red for illustrative purposes. Figure 3C - Deployment of coils within the aneurysm lumen. Figure 3D - Completed embolization of the aneurysm.

References
-
- Stevens, et al. The Role of Mechanical Ventilation in Acute Brain Injury. Neurol Clin. 2008:543–563. - PubMed
-
- Byyny, et al. Sensitivity of Noncontrast Cranial Computed Tomography for the Emergency Department Diagnosis of Subarachnoid Hemorrhage. Annals of Emergency Medicine. 51(6):697–703. - PubMed
-
- Greving, et al. Cost-effectiveness of preventative treatment of intracranial aneurysms. Neurology. 2009;73:258–265. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical