

Impact of routine percutaneous coronary intervention after out-of-hospital cardiac arrest due to ventricular fibrillation
- PMID: 21569361
- PMCID: PMC3218980
- DOI: 10.1186/cc10227
Impact of routine percutaneous coronary intervention after out-of-hospital cardiac arrest due to ventricular fibrillation
Abstract
Introduction: Since 2003, we have routinely used percutaneous coronary intervention (PCI) and mild therapeutic hypothermia (MTH) to treat patients < 80 years of age after out-of-hospital cardiac arrest (OHCA) related to ventricular fibrillation. The aim of our study was to evaluate the prognostic impact of routine PCI in association with MTH and the potential influence of age.
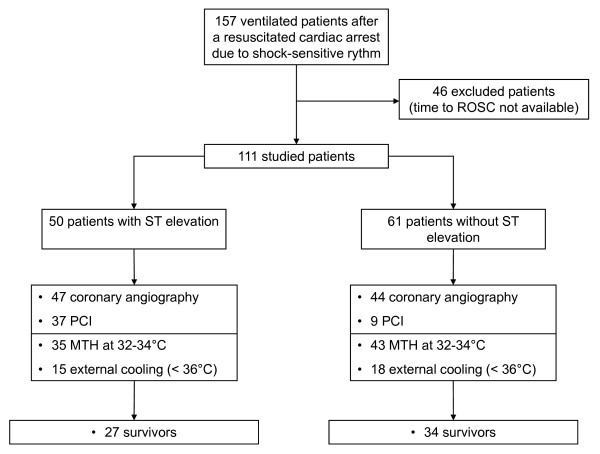
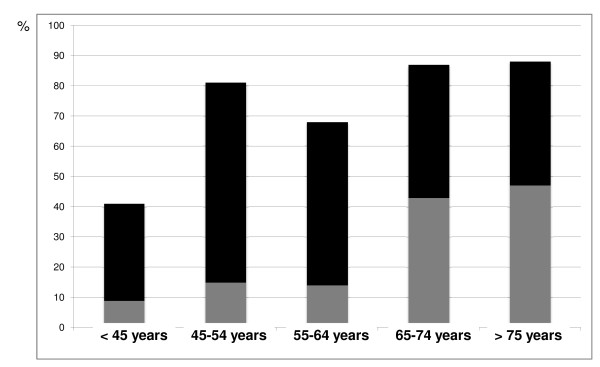
Methods: We studied 111 consecutive patients resuscitated successfully following OHCA related to shock-sensitive rhythm. They were divided into five groups according to age: < 45 years (n = 22, group 1), 45 to 54 years (n = 27, group 2), 55 to 64 years (n = 22, group 3), 65 to 74 years (n = 23, group 4) and ≥75 years (n = 17, group 5). Emergency coronary angiography was performed in hemodynamically stable patients < 80 years old, regardless of the electrocardiogram pattern. MTH was targeted to a core temperature of 32°C to 34°C for 24 hours.
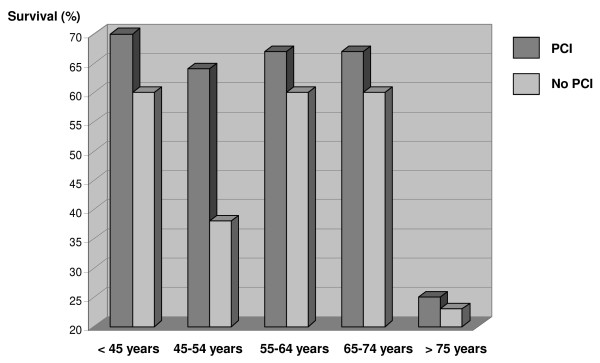
Results: Most patients (73%) had coronary heart disease, although its incidence in group 1 was lower than in other groups (41% versus 81%; P = 0.01). In group 1, all patients but one underwent coronary angiography, and 33% of them underwent associated PCI. In group 5, only 53% of patients underwent a coronary angiography and 44% underwent PCI. Overall in-hospital survival was 54%, ranging between 52% and 64% in groups 1 to 4 and 24% in group 5. Time from collapse to return of spontaneous circulation was associated with mortality (odds ratio (OR) = 1.05 (25th to 75th percentile range, 1.03 to 1.08); P < 0.001), whereas PCI was associated with survival (OR = 0.30 (25th to 75th percentile range, 0.11 to 0.79); P = 0.01).
Conclusions: We suggest that routine coronary angiography with potentially associated PCI may favorably alter the prognosis of resuscitated patients with stable hemodynamics who are treated with MTH after OHCA related to ventricular fibrillation. Although age was not an independent cause of death, the clinical relevance of this therapeutic strategy remains to be determined in older people.
Figures
Comment in
-
'Cooling and cathing' the post-resuscitated.Crit Care. 2011 Aug 8;15(4):178. doi: 10.1186/cc10299. Crit Care. 2011. PMID: 21888679 Free PMC article.
References
-
- Deakin CD, Morrison LJ, Morley PT, Callaway CW, Kerber RE, Kronick SL, Lavonas EJ, Link MS, Neumar RW, Otto CW, Parr M, Shuster M, Sunde K, Peberdy MA, Tang W, Hoek TL, Böttiger BW, Drajer S, Lim SH, Nolan JP. Advanced life support: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Advanced Life Support Chapter Collaborators. Resuscitation. 2010;81(Suppl 1):e93–e174. - PubMed
-
- Neumar RW, Nolan JP, Adrie C, Aibiki M, Berg RA, Böttiger BW, Callaway C, Clarks RS, Geocadin RG, Jauch EC, Kern KB, Laurent I, Longstrenth WT Jr, Merchant RM, Morley P, Morrison LJ, Nadkarni V, Peberdy MA, Rivers EP, Rodriguez-Nunez A, Selke FW, Spaulding C, Sunde K, Vanden Hoek T. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the international liaison committee on resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee, the Council of Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, perioperative, and critical care; the Council on Clinical Cardiology; and the Stroke Council. Circulation. 2008;118:2452–2483. doi: 10.1161/CIRCULATIONAHA.108.190652. - DOI - PubMed
-
- Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurological outcome after cardiac arrest. N Engl J Med. 2002;346:549–556. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
