

Revisiting the pathogenesis of podagra: why does gout target the foot?
- PMID: 21569453
- PMCID: PMC3117776
- DOI: 10.1186/1757-1146-4-13
Revisiting the pathogenesis of podagra: why does gout target the foot?
Abstract
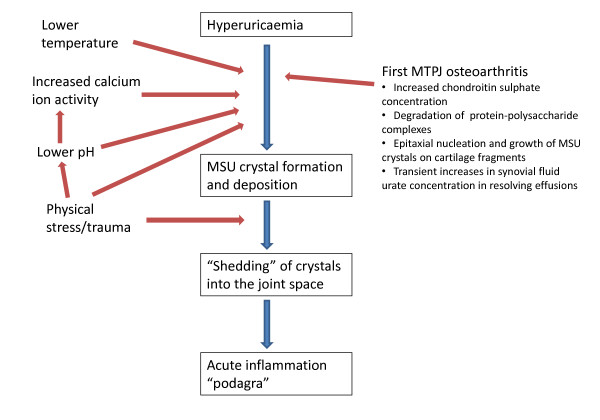
This invited paper provides a summary of a keynote lecture delivered at the 2011 Australasian Podiatry Conference. Gout is the most prevalent inflammatory arthropathy. It displays a striking predilection to affect the first metatarsophalangeal joint as well as joints within the mid-foot and ankle. A number of factors are known to reduce urate solubility and enhance nucleation of monosodium urate crystals including decreased temperature, lower pH and physical shock, all of which may be particularly relevant to crystal deposition in the foot. An association has also been proposed between monosodium urate crystal deposition and osteoarthritis, which also targets the first metatarsophalangeal joint. Cadaveric, clinical and radiographic studies indicate that monosodium urate crystals more readily deposit in osteoarthritic cartilage. Transient intra-articular hyperuricaemia and precipitation of monosodium urate crystals is thought to follow overnight resolution of synovial effusion within the osteoarthritic first metatarsophalangeal joint. The proclivity of gout for the first metatarsophalangeal joint is likely to be multi-factorial in origin, arising from the unique combination of the susceptibility of the joint to osteoarthritis and other determinants of urate solubility and crystal nucleation such as temperature and minor physical trauma which are particularly relevant to the foot.
Figures

References
-
- Porter R, Rousseau GS. Gout The Patrician Malady. New Haven and London: Yale University Press; 1998.
Grants and funding
LinkOut - more resources
Full Text Sources
