

Establishing a sentinel lymph node mapping algorithm for the treatment of early cervical cancer
- PMID: 21570713
- PMCID: PMC4996075
- DOI: 10.1016/j.ygyno.2011.04.023
Establishing a sentinel lymph node mapping algorithm for the treatment of early cervical cancer
Abstract
Objective: To establish an algorithm that incorporates sentinel lymph node (SLN) mapping to the surgical treatment of early cervical cancer, ensuring that lymph node (LN) metastases are accurately detected but minimizing the need for complete lymphadenectomy (LND).
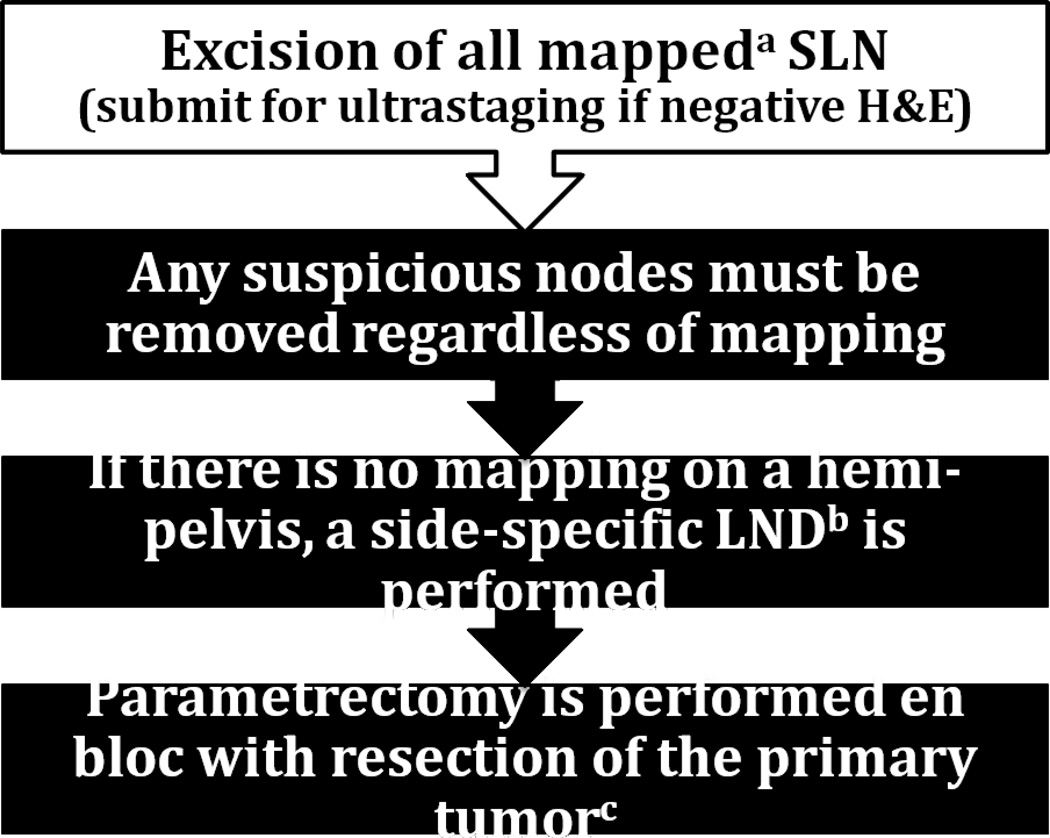
Methods: A prospectively maintained database of all patients who underwent SLN procedure followed by a complete bilateral pelvic LND for cervical cancer (FIGO stages IA1 with LVI to IIA) from 03/2003 to 09/2010 was analyzed. The surgical algorithm we evaluated included the following: 1. SLNs are removed and submitted to ultrastaging; 2. any suspicious LN is removed regardless of mapping; 3. if only unilateral mapping is noted, a contralateral side-specific pelvic LND is performed (including inter-iliac nodes); and 4. parametrectomy en bloc with primary tumor resection is done in all cases. We retrospectively applied the algorithm to determine how it would have performed.
Results: One hundred twenty-two patients were included. Median SLN count was 3 and median total LN count was 20. At least one SLN was identified in 93% of cases (114/122), while optimal (bilateral) mapping was achieved in 75% of cases (91/122). SLN correctly diagnosed 21 of 25 patients with nodal spread. When the algorithm was applied, all patients with LN metastasis were detected; with optimal mapping, bilateral pelvic LND could have been avoided in 75% of cases.
Conclusions: In the surgical treatment of early cervical cancer, the algorithm we propose allows for comprehensive detection of all patients with nodal disease and spares complete LND in the majority of cases.
Copyright © 2011 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Pecorelli S, Zigliani L, Odicino F. Revised FIGO staging for carcinoma of the cervix. Int J Gynaecol Obstet. 2009;105:107–108. - PubMed
-
- Creasman WT, Kohler MF. Is lymph vascular space involvement an independent prognostic factor in early cervical cancer? Gynecol Oncol. 2004;92:525–529. - PubMed
-
- Delgado G, Bundy B, Zaino R, Sevin BU, Creasman WT, Major F. Prospective surgical-pathological study of disease-free interval in patients with stage IB squamous cell carcinoma of the cervix: a Gynecologic Oncology Group study. Gynecol Oncol. 1990;38:352–357. - PubMed
-
- Yuan C, Wang P, Lai C, Tsu E, Yen M, Ng H. Recurrence and survival analyses of 1,115 cervical cancer patients treated with radical hysterectomy. Gynecol Obstet Invest. 1999;47:127–132. - PubMed
