

Imaging the electromechanical activity of the heart in vivo
- PMID: 21571641
- PMCID: PMC3102378
- DOI: 10.1073/pnas.1011688108
Imaging the electromechanical activity of the heart in vivo
Abstract
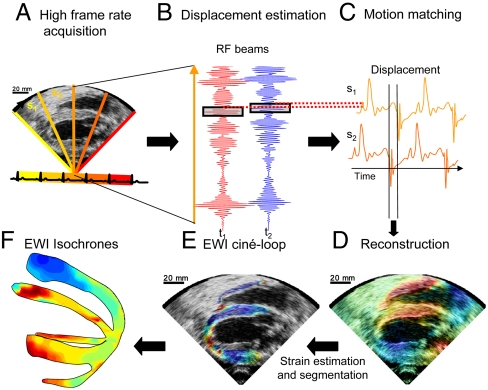
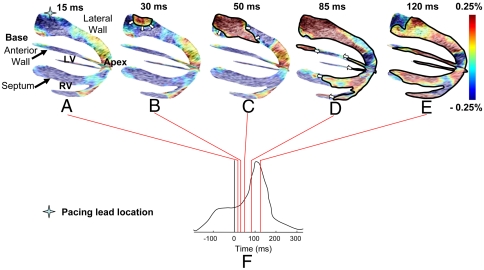
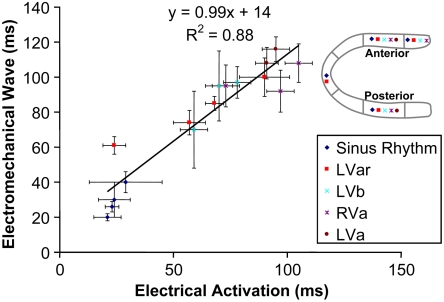
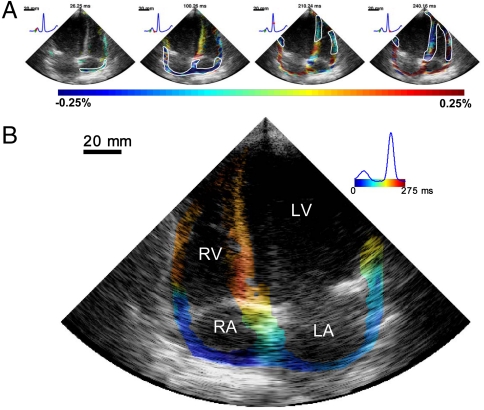
Cardiac conduction abnormalities remain a major cause of death and disability worldwide. However, as of today, there is no standard clinical imaging modality that can noninvasively provide maps of the electrical activation. In this paper, electromechanical wave imaging (EWI), a novel ultrasound-based imaging method, is shown to be capable of mapping the electromechanics of all four cardiac chambers at high temporal and spatial resolutions and a precision previously unobtainable in a full cardiac view in both animals and humans. The transient deformations resulting from the electrical activation of the myocardium were mapped in 2D and combined in 3D biplane ventricular views. EWI maps were acquired during five distinct conduction configurations and were found to be closely correlated to the electrical activation sequences. EWI in humans was shown to be feasible and capable of depicting the normal electromechanical activation sequence of both atria and ventricles. This validation of EWI as a direct, noninvasive, and highly translational approach underlines its potential to serve as a unique imaging tool for the early detection, diagnosis, and treatment monitoring of arrhythmias through ultrasound-based mapping of the transmural electromechanical activation sequence reliably at the point of care, and in real time.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Bers DM. Cardiac excitation-contraction coupling. Nature. 2002;415:198–205. - PubMed
-
- Cordeiro JM, Greene L, Heilmann C, Antzelevitch D, Antzelevitch C. Transmural heterogeneity of calcium activity and mechanical function in the canine left ventricle. Am J Physiol Heart Circ Physiol. 2004;286:H1471–H1479. - PubMed
-
- Zhang X, et al. Noninvasive three-dimensional electrocardiographic imaging of ventricular activation sequence. Am J Physiol Heart Circ Physiol. 2005;289:H2724–H2732. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
