

Preliminary classification criteria for the cryoglobulinaemic vasculitis
- PMID: 21571735
- PMCID: PMC3103668
- DOI: 10.1136/ard.2011.150755
Preliminary classification criteria for the cryoglobulinaemic vasculitis
Abstract
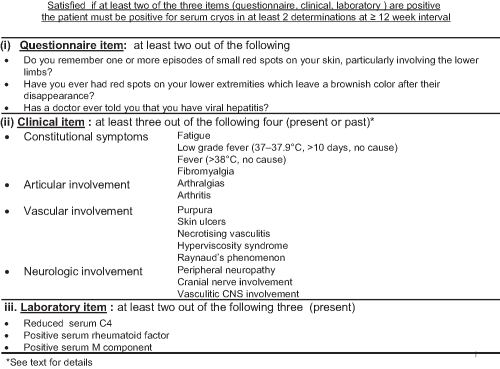
Background: To develop preliminary classification criteria for the cryoglobulinaemic syndrome or cryoglobulinaemic vasculitis (CV).
Methods: Study part I developed a questionnaire for CV to be included in the formal, second part (study part II). Positivity of serum cryoglobulins was defined by experts as an essential condition for CV classification. In study part II, a core set of classification items (questionnaire, clinical and laboratory items, as agreed) was tested in three groups of patients and controls-that is, group A (new patients with the CV), group B (controls with serum cryoglobulins but lacking CV) and group C (controls without serum cryoglobulins but with features which can be observed in CV).
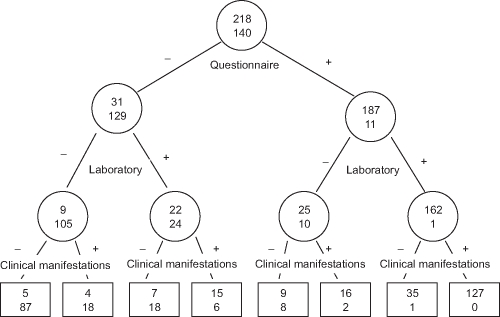
Results: In study part I (188 cases, 284 controls), a positive response to at least two of three selected questions showed a sensitivity of 81.9% and a specificity of 83.5% for CV. This questionnaire was employed and validated in study part II, which included 272 patients in group A and 228 controls in group B. The final classification criteria for CV, by pooling data from group A and group B, required the positivity of questionnaire plus clinical, questionnaire plus laboratory, or clinical plus laboratory items, or all the three, providing a sensitivity of 88.5% and a specificity of 93.6% for CV. By comparing data in group A versus group C (425 controls), the same classification criteria showed a sensitivity 88.5% and a specificity 97.0% for CV.
Conclusion: Classification criteria for CV were developed, and now need validation.
Figures
References
-
- Meltzer M, Franklin EC. Cryoglobulinemia – a study of twenty-nine patients. I. IgG and IgM cryoglobulins and factors affecting cryoprecipitability. Am J Med 1966;40:828–36 - PubMed
-
- Gorevic PD, Frangione B. Mixed cryoglobulinemia cross-reactive idiotypes: implications for the relationship of MC to rheumatic and lymphoproliferative diseases. Semin Hematol 1991;28:79–94 - PubMed
-
- De Vita S, De Re V, Gasparotto D, et al. Oligoclonal non-neoplastic B cell expansion is the key feature of type II mixed cryoglobulinemia: clinical and molecular findings do not support a bone marrow pathologic diagnosis of indolent B cell lymphoma. Arthritis Rheum 2000;43:94–102 - PubMed
-
- Ferri C, Greco F, Longombardo G, et al. Antibodies to hepatitis C virus in patients with mixed cryoglobulinemia. Arthritis Rheum 1991;34:1606–10 - PubMed
-
- Agnello V, Chung RT, Kaplan LM. A role for hepatitis C virus infection in type II cryoglobulinemia. N Engl J Med 1992;327:1490–5 - PubMed
