

Association between timing of antibiotic administration and mortality from septic shock in patients treated with a quantitative resuscitation protocol
- PMID: 21572327
- PMCID: PMC3158284
- DOI: 10.1097/CCM.0b013e31821e87ab
Association between timing of antibiotic administration and mortality from septic shock in patients treated with a quantitative resuscitation protocol
Abstract
Objective: We sought to determine the association between time to initial antibiotics and mortality of patients with septic shock treated with an emergency department-based early resuscitation protocol.
Design: Preplanned analysis of a multicenter randomized controlled trial of early sepsis resuscitation.
Setting: Three urban U.S. emergency departments.
Patients: Adult patients with septic shock.
Interventions: A quantitative resuscitation protocol in the emergency department targeting three physiological variables: central venous pressure, mean arterial pressure, and either central venous oxygen saturation or lactate clearance. The study protocol was continued until all end points were achieved or a maximum of 6 hrs.
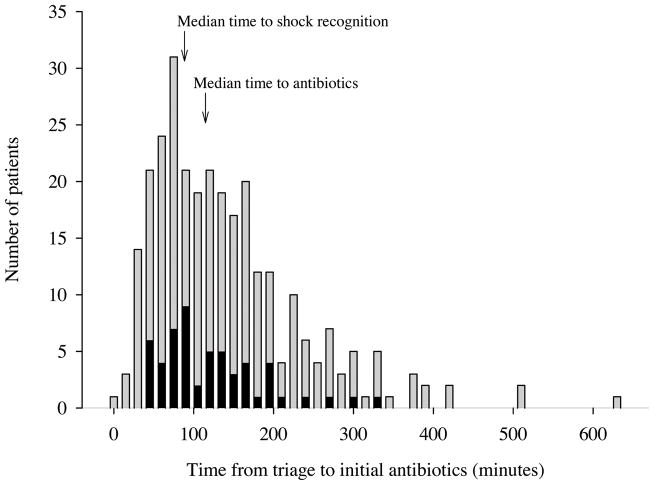
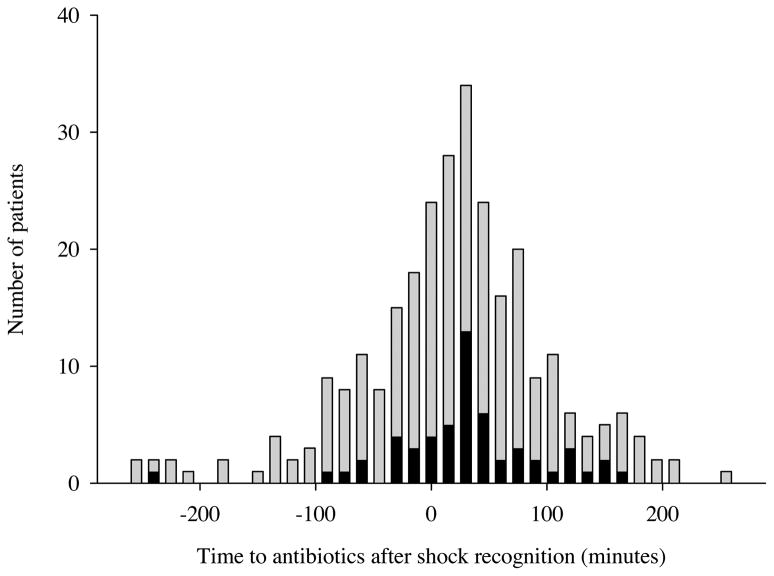
Measurements and main results: Data on patients who received an initial dose of antibiotics after presentation to the emergency department were categorized based on both time from triage and time from shock recognition to initiation of antibiotics. The primary outcome was inhospital mortality. Of 291 included patients, mortality did not change with hourly delays in antibiotic administration up to 6 hrs after triage: 1 hr (odds ratio [OR], 1.2; 0.6-2.5), 2 hrs (OR, 0.71; 0.4-1.3), 3 hrs (OR, 0.59; 0.3-1.3). Mortality was significantly increased in patients who received initial antibiotics after shock recognition (n = 172 [59%]) compared with before shock recognition (OR, 2.4; 1.1-4.5); however, among patients who received antibiotics after shock recognition, mortality did not change with hourly delays in antibiotic administration.
Conclusion: In this large, prospective study of emergency department patients with septic shock, we found no increase in mortality with each hour delay to administration of antibiotics after triage. However, delay in antibiotics until after shock recognition was associated with increased mortality.
Conflict of interest statement
The remaining authors have not disclosed any potential conflicts of interest.
Figures
Comment in
-
Antibiotics in sepsis: Timing, appropriateness, and (of course) timely recognition of appropriateness.Crit Care Med. 2011 Sep;39(9):2184-6. doi: 10.1097/CCM.0b013e3182226ffa. Crit Care Med. 2011. PMID: 21849829 No abstract available.
-
Should we or should we not allow delays in antimicrobial administration? Of course not!Crit Care Med. 2012 Mar;40(3):1035; author reply 1035-6. doi: 10.1097/CCM.0b013e31823dae6f. Crit Care Med. 2012. PMID: 22343877 No abstract available.
References
-
- Angus D, Linde-Zwirble W, Lidicker J, et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29(7):1303–1310. - PubMed
-
- Dombrovskiy VY, Martin AA, Sunderram J, et al. Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: A trend analysis from 1993 to 2003. Crit Care Med. 2007;35(5):1244–1250. - PubMed
-
- Wang HE, Shapiro NI, Angus DC, et al. National estimates of severe sepsis in United States emergency departments. Crit Care Med. 2007;35(8):1928–1936. - PubMed
-
- Dellinger RP, Levy MM, Carlet JM, et al. Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008;36(1):296–327. - PubMed
-
- Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34(6):1589–1596. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
