

doi: 10.4103/1817-1737.78412.
Pulmonary vascular complications of chronic liver disease: Pathophysiology, imaging, and treatment
Affiliations
- PMID: 21572693
- PMCID: PMC3081557
- DOI: 10.4103/1817-1737.78412
Item in Clipboard
Pulmonary vascular complications of chronic liver disease: Pathophysiology, imaging, and treatment
Ann Thorac Med.
2011 Apr.
Abstract
To review the pathogenesis of pulmonary vascular complications of liver disease, we discuss their clinical implications, and therapeutic considerations, with emphasis on potential reversibility of the hepatopulmonary syndrome after liver transplantation. In this review, we also discuss the role of imaging in pulmonary vascular complications associated with liver disease.
Keywords: Hepatopulmonary syndrome; Yttrium-90 microsphere embolization hepatocellular carcinoma; portopulmonary hypertension; pulmonary arteriovenous shunts.
Conflict of interest statement
Figures
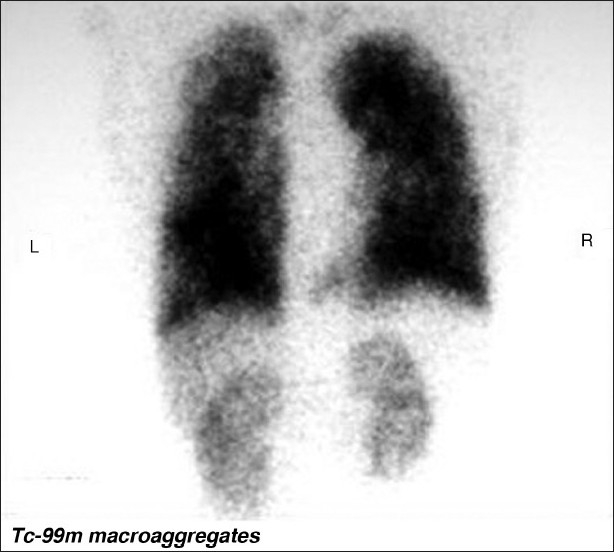
99Technetium macroaggregated albumin perfusion imaging in a patient with HPS shows a right to left shunt. The 99mTc-MMA has entered the systemic circulation and has perfused the kidneys
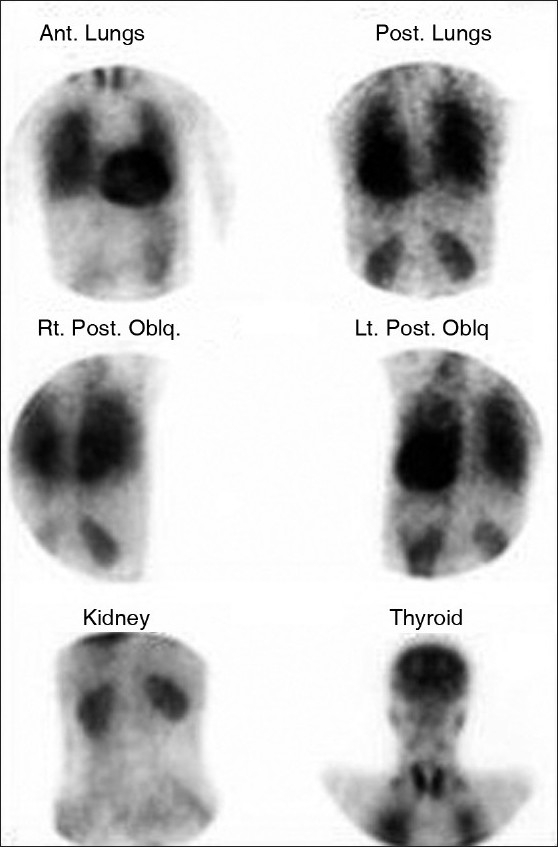
99Technetium macroaggregated albumin perfusion imaging in a patient with HPS shows a right to left shunt. The 99mTc-MMA has entered the systemic circulation and distributed to systemic organs. Normally, <5% of the isotope can be quantitated over the brain. In HPS, there is >6% uptake in the brain as in this case. (Courtesy Durre-e-Sabih Multan)
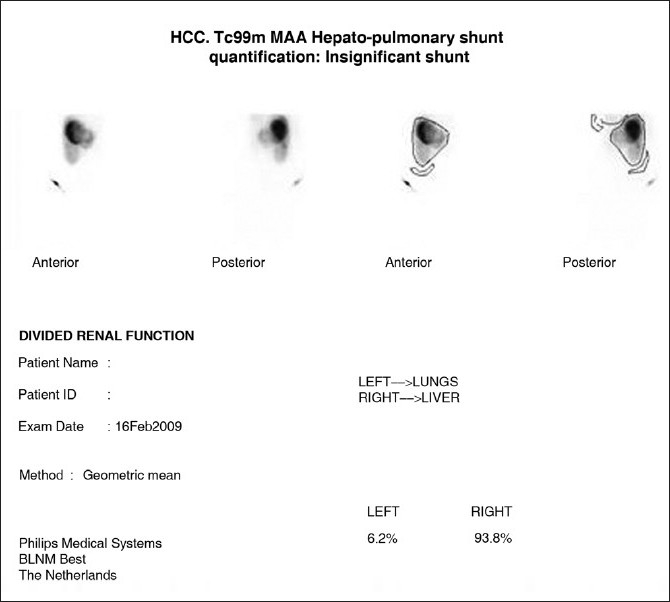
In preparation for hepatic radioembolization with Yttrium-90 glass microspheres 99Technetium macroaggregated is given via the hepatic artery and regions of interest are drawn over lungs, liver and background. Less than 5% systemic shunt of 99Technetium macroaggregated is normal. The 5–15% is insignificant and we proceed to Yttrium-90 glass microspheres with a standard 150 Gy dose. With a systemic shunt of 10–25%, the dose of Yttrium-90 glass microspheres is modified to 110-130 Gys. (Courtesy Dr. Ghulam Mustafa Shah, Department of Medical King Abdul Aziz Medical City Riyadh)
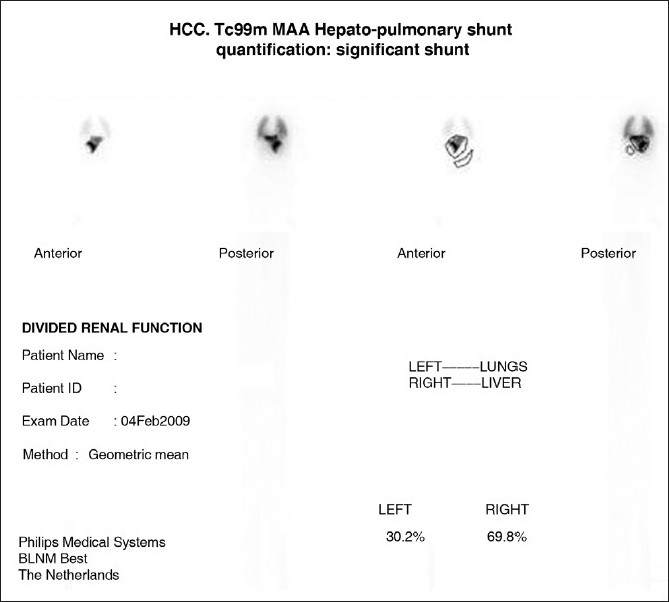
In preparation for hepatic radioembolization with Yttrium-90 glass microspheres 99Technetium macroaggregated is given via the hepatic artery and regions of interest are drawn over lungs, liver, and background. With a systemic shunt greater than 25% Yttrium-90 glass microspheres embolization is contraindicated. (Courtesy Dr. Ghulam Mustafa Shah Syed, Head Nuclear Medicine Section, Department of Medical Imaging, King Fahad Hospital, King Abdul Aziz Medical City Riyadh)

A coned view of a CXR of lung basis with HPS shows bibasilar nodular or reticulonodular opacities. These are seen in 5–13.8% of patients with CLD and 46–100% of patients with HPS. These opacities are shown to represent dilated lung vessels on computed tomography as shown
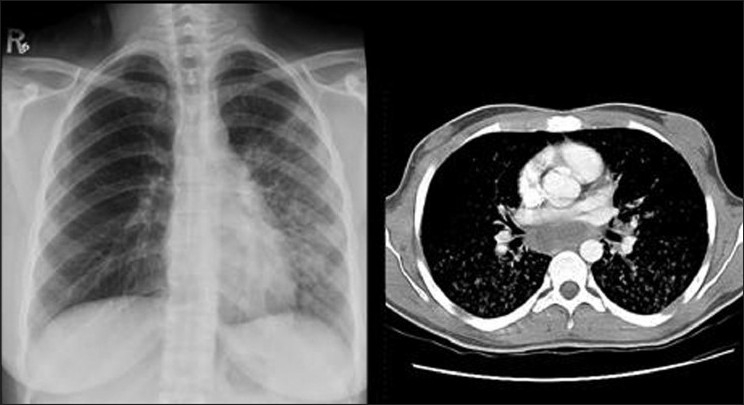
A CXR of lung basis of 47-year-old woman with HPS shows basilar reticulonodular opacities at the left lung base and left mid-zone. These opacities which represent dilated lung vessels are seen on both sides on CT as shown
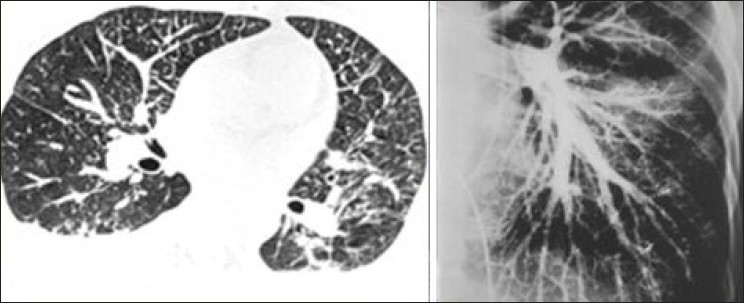
Axial contrast enhanced CT (right) and a pulmonary angiogram (left) show dilated pulmonary vasculature in a 53-year-old man with CLD associated with HPS
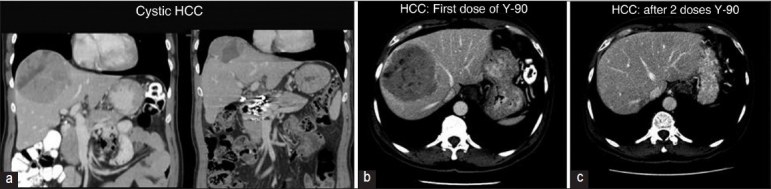
(a) Illustrate the application of hepatic radioembolization with Yttrium-90 glass microspheres 99Technetium following quantitative estimation of a right to left intracardiac shunt by a 99Technetium macroaggregated perfusion lung scan. These series of images (b, c) illustrate the benefit of hepatic radioembolization with Yttrium-90 glass microspheres in a cystic hepatocellular carcinoma. There is an initial necrosis of the tumor followed by almost complete shrinkage. (Courtesy Dr Ghulam Mustafa Shah Syed, Department of Medical Imaging, Abdul Aziz Medical City Riyadh)
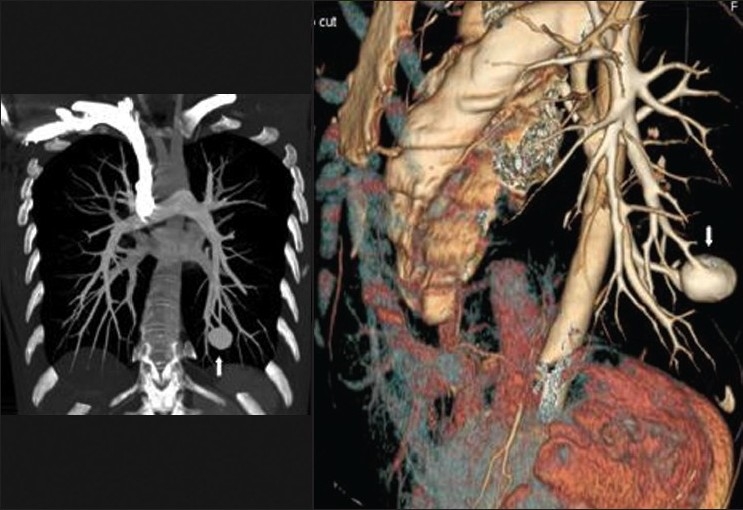
It is important that larger right to left shunts through pulmonary arteriovenous malformations are excluded by cross-sectional imaging when testing for HPS and when consideration is being given for hepatic radioembolization with Yttrium-90 glass microspheres. These coronal and sagittal reconstructions of contrast enhanced CT show a large arteriovenous malformation at the left lung base
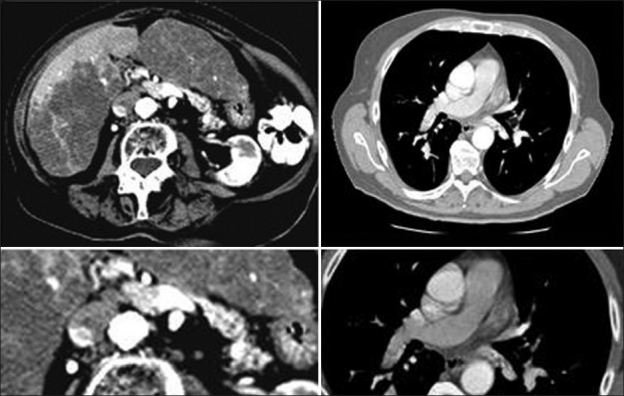
Axial contrast enhanced images of the liver and lungs on an 82-year-old woman with PPH showing portal vein thrombosis, which is associated with pulmonary embolism supporting the theory that PPH may be secondary to embolic material entering the lungs via the portosystemic venous shunts associated with PoH although no varices are seen in this patient
A CXR of a 41-year-old man with cirrhosis and PPH show enlarged hila and peripheral pruning of the vessels secondary to PH. An axial contrast enhanced CT through the pulmonary arteries of another patient with PPH showing aneurismal dilatation of the main pulmonary artery and the right pulmonary artery with peripheral pruning due to PH

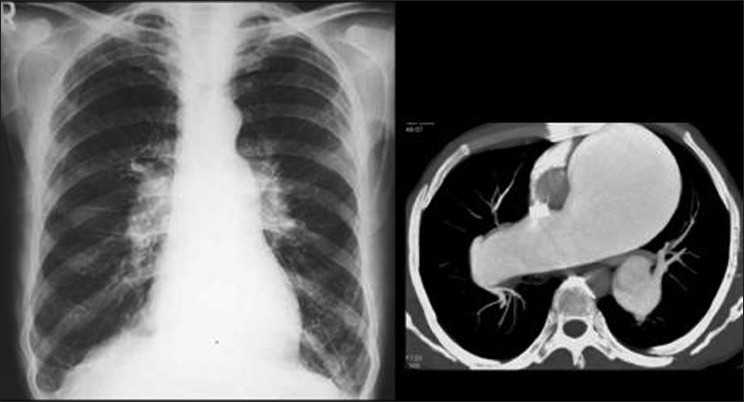
A CXR on a patient with PPH secondary to cirrhosis shows a dilated pulmonary conus and aneurismal dilatation of the right pulmonary artery. The image on the left is coronal reconstruction of contrast enhanced CT on the same patient, which depicts a probable re-canalized thrombus underlying the aneurismal dilatation of the right pulmonary artery

Pulmonary angiography on a patient with PPH showing dilatation of the pulmonary arteries and pruning of the peripheral vessels
Similar articles
-
Hepatopulmonary syndrome and portopulmonary hypertension.Hepatol Res. 2009 Oct;39(10):1020-2. doi: 10.1111/j.1872-034X.2009.00552.x. Hepatol Res. 2009. PMID: 19796040
-
Hepatopulmonary syndrome and portopulmonary hypertension: recent knowledge in pathogenesis and overview of clinical assessment.Liver Int. 2015 Jun;35(6):1646-60. doi: 10.1111/liv.12791. Epub 2015 Feb 16. Liver Int. 2015. PMID: 25627425 Review.
-
Coexisting hepatopulmonary syndrome and portopulmonary hypertension: implications for liver transplantation.J Clin Gastroenterol. 2010 Aug;44(7):e136-40. doi: 10.1097/MCG.0b013e3181da76fc. J Clin Gastroenterol. 2010. PMID: 20463591
-
Severe portopulmonary hypertension after liver transplantation in a patient with preexisting hepatopulmonary syndrome.J Hepatol. 1999 Dec;31(6):1075-9. doi: 10.1016/s0168-8278(99)80321-3. J Hepatol. 1999. PMID: 10604582
-
Pulmonary vascular disorders in portal hypertension.Eur Respir J. 1998 May;11(5):1153-66. doi: 10.1183/09031936.98.11051153. Eur Respir J. 1998. PMID: 9648972 Review.
Cited by
-
The end-organ impairment in liver cirrhosis: appointments for critical care.Crit Care Res Pract. 2012;2012:539412. doi: 10.1155/2012/539412. Epub 2012 May 16. Crit Care Res Pract. 2012. PMID: 22666568 Free PMC article.
-
Cirrhosis and hepatopulmonary syndrome.World J Gastroenterol. 2014 Mar 14;20(10):2586-94. doi: 10.3748/wjg.v20.i10.2586. World J Gastroenterol. 2014. PMID: 24627594 Free PMC article. Review.
-
Assessing the kinetics of microbubble appearance in cirrhotic patients using transthoracic saline contrast-enhanced echocardiography.Echocardiography. 2017 Oct;34(10):1439-1446. doi: 10.1111/echo.13662. Epub 2017 Aug 25. Echocardiography. 2017. PMID: 28840954 Free PMC article.
-
Pulmonary Complications in Candidates for Liver Transplantation.Middle East J Dig Dis. 2020 Jul;12(3):145-153. doi: 10.34172/mejdd.2020.176. Middle East J Dig Dis. 2020. PMID: 33062219 Free PMC article. Review.
-
Supine vs upright exercise in patients with hepatopulmonary syndrome and orthodeoxia: study protocol for a randomized controlled crossover trial.Trials. 2021 Oct 9;22(1):683. doi: 10.1186/s13063-021-05633-7. Trials. 2021. PMID: 34625098 Free PMC article.
References
-
- Krowka MJ, Cortese DA. Hepatopulmonary syndrome: An evolving perspective in the era of liver transplantation. Hepatology. 1990;11:138–42. - PubMed
-
- Kennedy TC, Knudson RJ. Exercise-aggravated hypoxemia and orthodexia in cirrhosis. Chest. 1997;72:305–9. - PubMed
-
- Krowka MJ, Cortese DA. Hepatopulmonary syndrome: Current concepts in diagnostic and therapeutic considerations. Chest. 1994;105:1528–37. - PubMed
-
- Abrams GA, Jaffe CC, Hoffer PB, Binder HJ, Fallon MB. Diagnostic utility of contrast echocardiography and lung perfusion scan in patients with hepatopulmonary syndrome. Gastroenterology. 1995;109:1283–8. - PubMed
-
- Castro M, Krowka MJ. Hepatopulmonary syndrome: A pulmonary vascular complication of liver disease. Clin Chest Med. 1996;17:35–48. - PubMed
