

Efficacy and safety of single and double doses of ivermectin versus 7-day high dose albendazole for chronic strongyloidiasis
- PMID: 21572981
- PMCID: PMC3091835
- DOI: 10.1371/journal.pntd.0001044
Efficacy and safety of single and double doses of ivermectin versus 7-day high dose albendazole for chronic strongyloidiasis
Abstract
Background: Strongyloidiasis, caused by an intestinal helminth Strongyloides stercoralis, is common throughout the tropics. It remains an important health problem due to autoinfection, which may result in hyperinfection and disseminated infection in immunosuppressed patients, especially patients receiving chemotherapy or corticosteroid treatment. Ivermectin and albendazole are effective against strongyloidiasis. However, the efficacy and the most effective dosing regimen are to be determined.
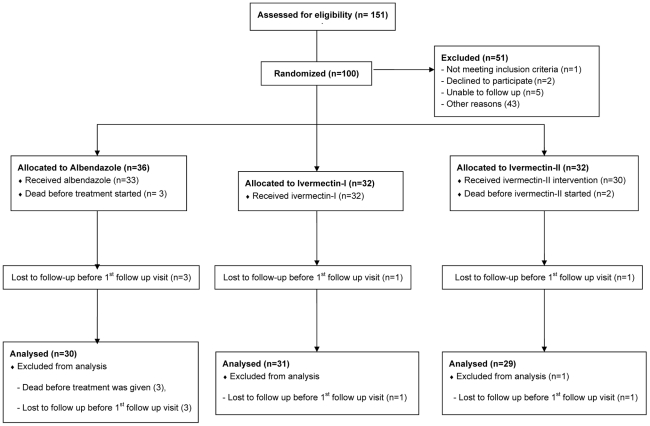
Methods: A prospective, randomized, open study was conducted in which a 7-day course of oral albendazole 800 mg daily was compared with a single dose (200 microgram/kilogram body weight), or double doses, given 2 weeks apart, of ivermectin in Thai patients with chronic strongyloidiasis. Patients were followed-up with 2 weeks after initiation of treatment, then 1 month, 3 months, 6 months, 9 months, and 1 year after treatment. Combination of direct microscopic examination of fecal smear, formol-ether concentration method, and modified Koga agar plate culture were used to detect strongyloides larvae in two consecutive fecal samples in each follow-up visit. The primary endpoint was clearance of strongyloides larvae from feces after treatment and at one year follow-up.
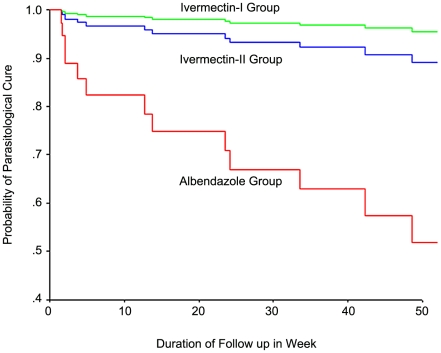
Results: Ninety patients were included in the analysis (30, 31 and 29 patients in albendazole, single dose, and double doses ivermectin group, respectively). All except one patient in this study had at least one concomitant disease. Diabetes mellitus, systemic lupus erythrematosus, nephrotic syndrome, hematologic malignancy, solid tumor and human immunodeficiency virus infection were common concomitant diseases in these patients. The median (range) duration of follow-up were 19 (2-76) weeks in albendazole group, 39 (2-74) weeks in single dose ivermectin group, and 26 (2-74) weeks in double doses ivermectin group. Parasitological cure rate were 63.3%, 96.8% and 93.1% in albendazole, single dose oral ivermectin, and double doses of oral ivermectin respectively (P = 0.006) in modified intention to treat analysis. No serious adverse event associated with treatment was found in any of the groups.
Conclusion/significance: This study confirms that both a single, and a double dose of oral ivermectin taken two weeks apart, is more effective than a 7-day course of high dose albendazole for patients with chronic infection due to S. stercoralis. Double dose of ivermectin, taken two weeks apart, might be more effective than a single dose in patients with concomitant illness.
Trial registration: ClinicalTrials.gov NCT00765024.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Bethony J, Brooker S, Albonico M, Geiger SM, Loukas A, et al. Soil-transmitted helminth infections: ascariasis, trichuriasis, and hookworm. Lancet. 2006;367:1521–1532. - PubMed
-
- Sithithaworn P, Srisawangwong T, Tesana S, Daenseekaew W, Sithithaworn J, et al. Epidemiology of Strongyloides stercoralis in north-east Thailand: application of the agar plate culture technique compared with the enzyme-linked immunosorbent assay. Trans R Soc Trop Med Hyg. 2003;97:398–402. - PubMed
-
- Concha R, Harrington W, Rogers AI. Intestinal strongyloidiasis: recognition, management, and determinants of outcomes. J Clin Gastroenterol. 2005;39:203–211. - PubMed
-
- Hirata T, Uchima N, Kishimoto K, Zaha O, Kinjo N, et al. Impairment of host immune response against Strongyloides stercoralis by human T cell lymphotropic virus type 1 infection. Am J Trop Med Hyg. 2006;74:246–9. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
