

The statistical pitfalls of the partially randomized preference design in non-blinded trials of psychological interventions
- PMID: 21574206
- PMCID: PMC6878315
- DOI: 10.1002/mpr.326
The statistical pitfalls of the partially randomized preference design in non-blinded trials of psychological interventions
Abstract
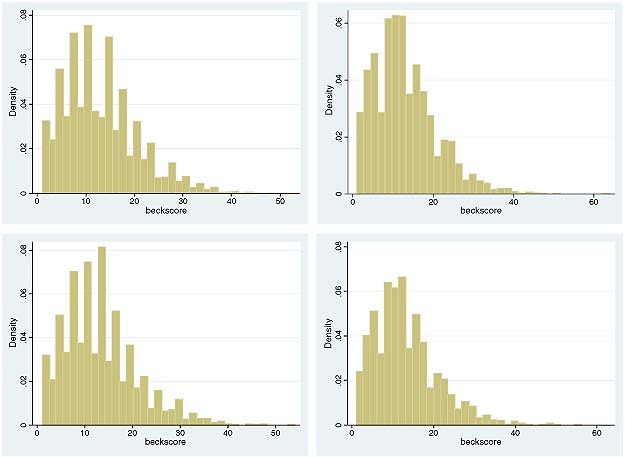
In a partially randomized preference trial (PRPT) patients with no treatment preference are allocated to groups at random, but those who express a preference receive the treatment of their choice. It has been suggested that the design can improve the external and internal validity of trials. We used computer simulation to illustrate the impact that an unmeasured confounder could have on the results and conclusions drawn from a PRPT. We generated 4000 observations ("patients") that reflected the distribution of the Beck Depression Index (DBI) in trials of depression. Half were randomly assigned to a randomized controlled trial (RCT) design and half were assigned to a PRPT design. In the RCT, "patients" were evenly split between treatment and control groups; whereas in the preference arm, to reflect patient choice, 87.5% of patients were allocated to the experimental treatment and 12.5% to the control. Unadjusted analyses of the PRPT data consistently overestimated the treatment effect and its standard error. This lead to Type I errors when the true treatment effect was small and Type II errors when the confounder effect was large. The PRPT design is not recommended as a method of establishing an unbiased estimate of treatment effect due to the potential influence of unmeasured confounders.
Copyright © 2011 John Wiley & Sons, Ltd.
References
-
- Beck A., Ward C., Mendelson M. (1961) An inventory for measuring depression. Archives of General Psychiatry, 4, 561–571. - PubMed
-
- Bedi N., Chilvers C., Churchill R., Dewey M., Duggan C., Fielding K., Gretton V., Miller P., Harrison G., Lee A., Williams I. (2000) Assessing effectiveness of treatment of depression in primary care – partially randomised preference trial. British Journal of Psychiatry, 177, 312–318. - PubMed
-
- Bower P., Byford S., Barber J., Beecham J., Simpson S., Friedli K., Corney R., King M., Harvey I. (2003) meta‐analysis of data on costs from trials of counselling in primary care: using individual patient data to overcome sample size limitations in economic analysis. British Medical Journal, 326, 1247–1250. - PMC - PubMed
-
- Bradley C. (1998) Designing medical and educational intervention studies. Diabetes Care, 16, 509–518. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
