

Prone position and recruitment manoeuvre: the combined effect improves oxygenation
- PMID: 21575205
- PMCID: PMC3218988
- DOI: 10.1186/cc10235
Prone position and recruitment manoeuvre: the combined effect improves oxygenation
Abstract
Introduction: Among the various methods for improving oxygenation while decreasing the risk of ventilation-induced lung injury in patients with acute respiratory distress syndrome (ARDS), a ventilation strategy combining prone position (PP) and recruitment manoeuvres (RMs) can be practiced. We studied the effects on oxygenation of both RM and PP applied in early ARDS patients.
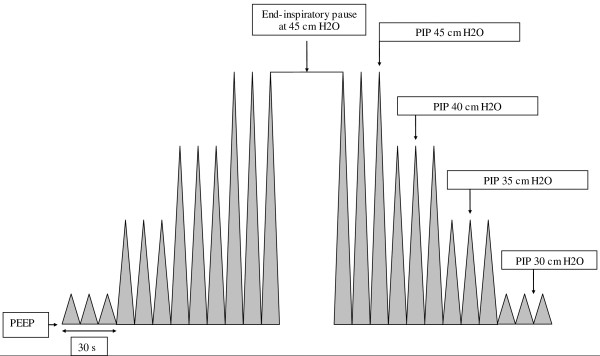
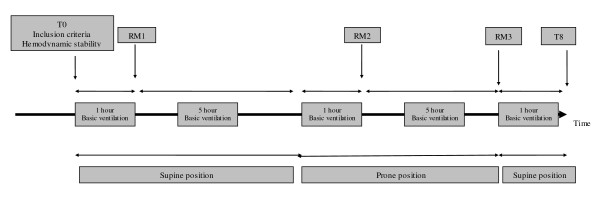
Methods: We conducted a prospective study. Sixteen consecutive patients with early ARDS fulfilling our criteria (ratio of arterial oxygen partial pressure to fraction of inspired oxygen (PaO2/FiO2) 98.3 ± 28 mmHg; positive end expiratory pressure, 10.7 ± 2.8 cmH2O) were analysed. Each patient was ventilated in both the supine position (SP) and the PP (six hours in each position). A 45 cmH2O extended sigh in pressure control mode was performed at the beginning of SP (RM1), one hour after turning to the PP (RM2) and at the end of the six-hour PP period (RM3).
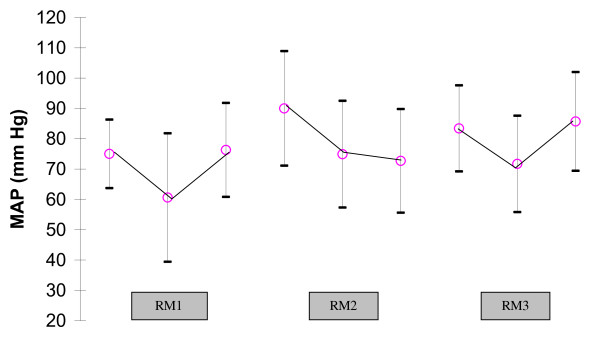
Results: The mean arterial oxygen partial pressure (PaO2) changes after RM1, RM2 and RM3 were 9.6%, 15% and 19%, respectively. The PaO2 improvement after a single RM was significant after RM3 only (P < 0.05). Improvements in PaO2 level and PaO2/FiO2 ratio were transient in SP but durable during PP. PaO2/FiO2 ratio peaked at 218 mmHg after RM3. PaO2/FiO2 changes were significant only after RM3 and in the pulmonary ARDS group (P = 0.008). This global strategy had a benefit with regard to oxygenation: PaO2/FiO2 ratio increased from 98.3 mmHg to 165.6 mmHg 13 hours later at the end of the study (P < 0.05). Plateau airway pressures decreased after each RM and over the entire PP period and significantly after RM3 (P = 0.02). Some reversible side effects such as significant blood arterial pressure variations were found when extended sighs were performed.
Conclusions: In our study, interventions such as a 45 cmH2O extended sigh during PP resulted in marked oxygenation improvement. Combined RM and PP led to the highest increase in PaO2/FiO2 ratio without major clinical side effects.
Figures
References
-
- Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy L, Legall JR, Morris A, Spragg R. The American-European Consensus Conference on ARDS: definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994;149:818–824. - PubMed
-
- Dreyfuss D, Saumon G. Ventilator-induced lung injury: lessons from experimental studies. Am J Respir Crit Care Med. 1998;157:294–323. - PubMed
-
- Ricard JD, Dreyfuss D, Saumon G. Ventilator induced lung injury. Eur Respir J Suppl. 2003;42:2s–9s. - PubMed
-
- Brochard L, Roudot-Thoraval F, Roupie E, Declaux C, Chastre J, Fernandez-Mondéjar E, Clémenti E, Mancebo J, Matamis D, Ranieri M, Blanch L, Rodi G, Mentec H, Dreyfuss D, Ferrer M, Brun-Buisson C, Tobin M, Lemaire F. Tidal volume reduction for prevention of ventilation-induced lung injury in acute respiratory distress syndrome. Am J Respir Crit Care Med. 1998;158:1831–1838. - PubMed
-
- The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
