

Systemic and vascular inflammation in patients with moderate to severe psoriasis as measured by [18F]-fluorodeoxyglucose positron emission tomography-computed tomography (FDG-PET/CT): a pilot study
- PMID: 21576552
- PMCID: PMC3158301
- DOI: 10.1001/archdermatol.2011.119
Systemic and vascular inflammation in patients with moderate to severe psoriasis as measured by [18F]-fluorodeoxyglucose positron emission tomography-computed tomography (FDG-PET/CT): a pilot study
Abstract
Objective: To evaluate the feasibility of using [18F]-fluorodeoxyglucose positron emission tomography-computed tomography (FDG-PET/CT) to detect and quantify systemic inflammation in patients with psoriasis.
Design: Case series with a nested case-control study.
Setting: Referral dermatology and preventive cardiology practices.
Participants: Six patients with psoriasis affecting more than 10% of their body surface area and 4 controls age and sex matched to 4 of the patients with psoriasis for a nested case-control study.
Main outcome measures: The FDG uptake in the liver, musculoskeletal structures, and aorta measured by mean standardized uptake value, a measure of FDG tracer uptake by macrophages and other inflammatory cells.
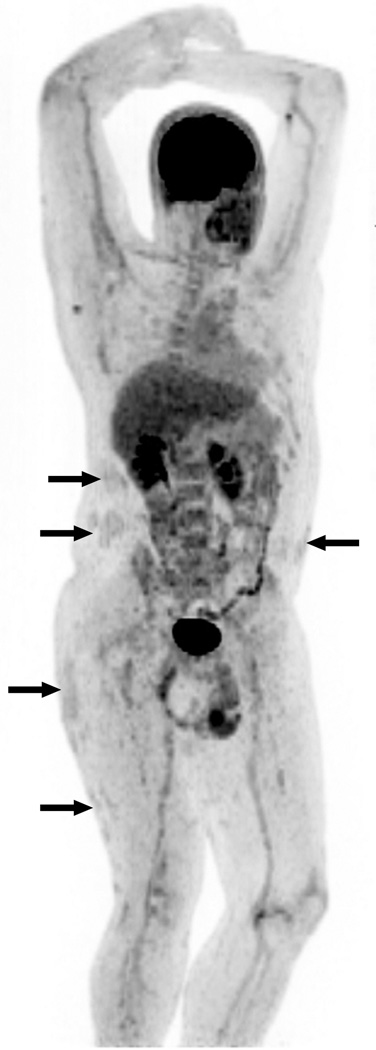
Results: FDG-PET/CT identified numerous foci of inflammation in 6 patients with psoriasis within the skin, liver, joints, tendons, and aorta. Inflammation in the joints was observed in a patient with psoriatic arthritis as well as in 1 patient with no history of joint disease or joint symptoms. In a nested case-control study, FDG-PET/CT imaging demonstrated increased vascular inflammation in multiple segments of the aorta compared with controls. These findings persisted after adjustment for traditional cardiovascular risk factors in multivariate analysis (mean β = 0.33; P < .001). Patients with psoriasis further demonstrated increased hepatic inflammation after adjusting for cardiovascular risk factors (β = 0.18; P < .001), but the association was no longer significant when adjusted for alcohol intake (β = -0.25; P = .07).
Conclusion: FDG-PET/CT is a sensitive tool for identifying inflammation and can be used to identify clinically observed inflammation in the skin and subclinical inflammation in the blood vessels, joints, and liver of patients with psoriasis.
Figures




References
-
- Gelfand JM, Weinstein R, Porter SB, Neimann AL, Berlin JA, Margolis DJ. Prevalence and treatment of psoriasis in the United Kingdom: a population-based study. Arch Dermatol. 2005 Dec;141(12):1537–1541. - PubMed
-
- Gelfand JM, Gladman DD, Mease PJ, et al. Epidemiology of psoriatic arthritis in the population of the United States. J Am Acad Dermatol. 2005 Oct;53(4):573. - PubMed
-
- Brauchli YB, Jick SS, Meier CR. Psoriasis and the risk of incident diabetes mellitus: a population-based study. Br J Dermatol. 2008 Sep 6; - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
