

Renin-angiotensin-aldosterone genotype influences ventricular remodeling in infants with single ventricle
- PMID: 21576655
- PMCID: PMC3137902
- DOI: 10.1161/CIRCULATIONAHA.110.004341
Renin-angiotensin-aldosterone genotype influences ventricular remodeling in infants with single ventricle
Abstract
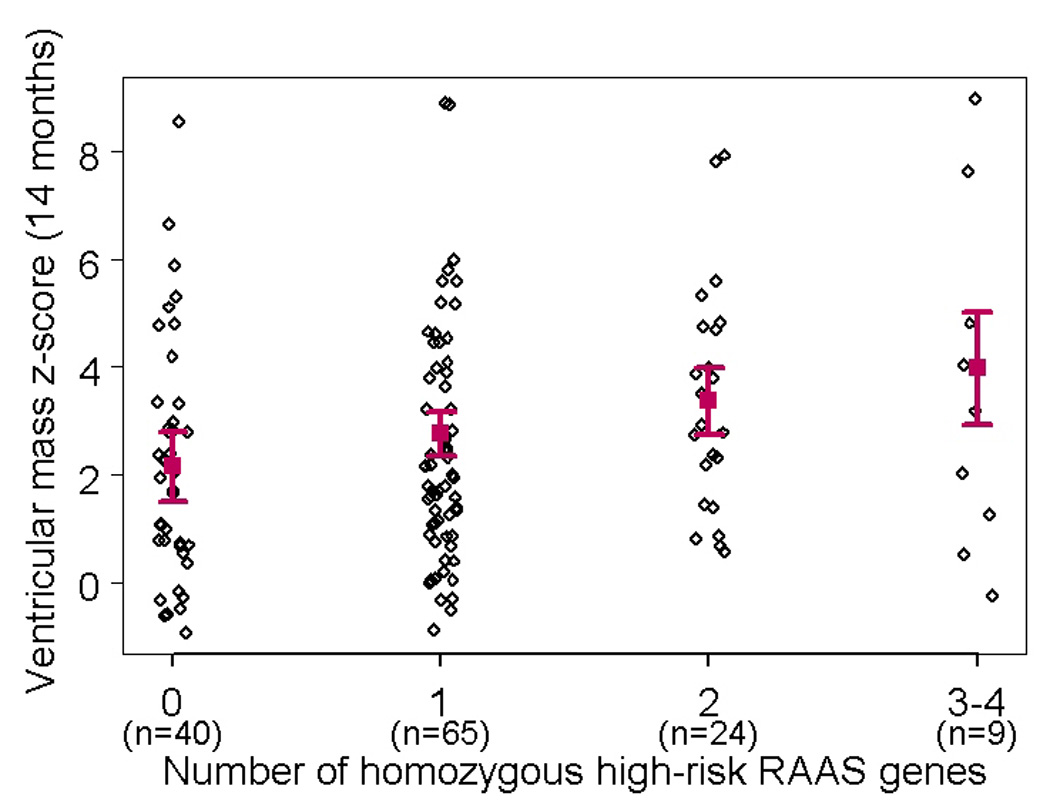
Background: We investigated the effect of polymorphisms in the renin-angiotensin-aldosterone system (RAAS) genes on ventricular remodeling, growth, renal function, and response to enalapril in infants with single ventricle.
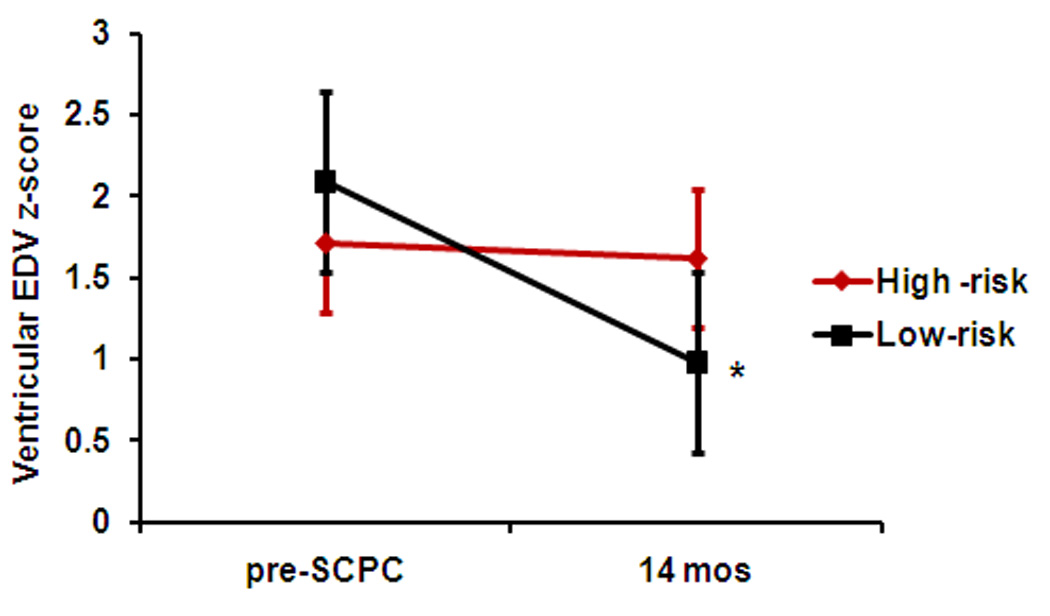
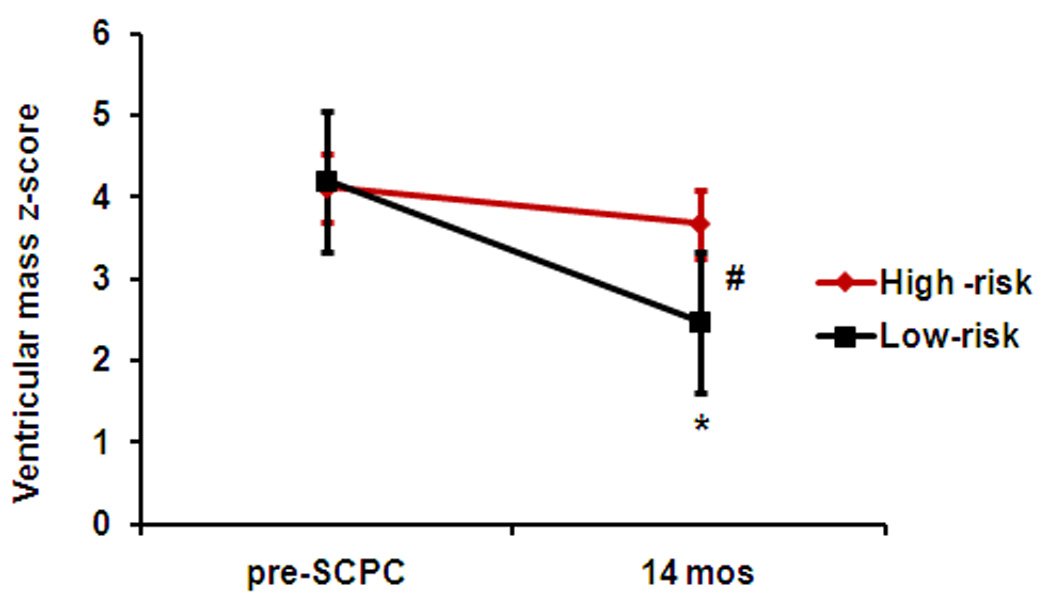
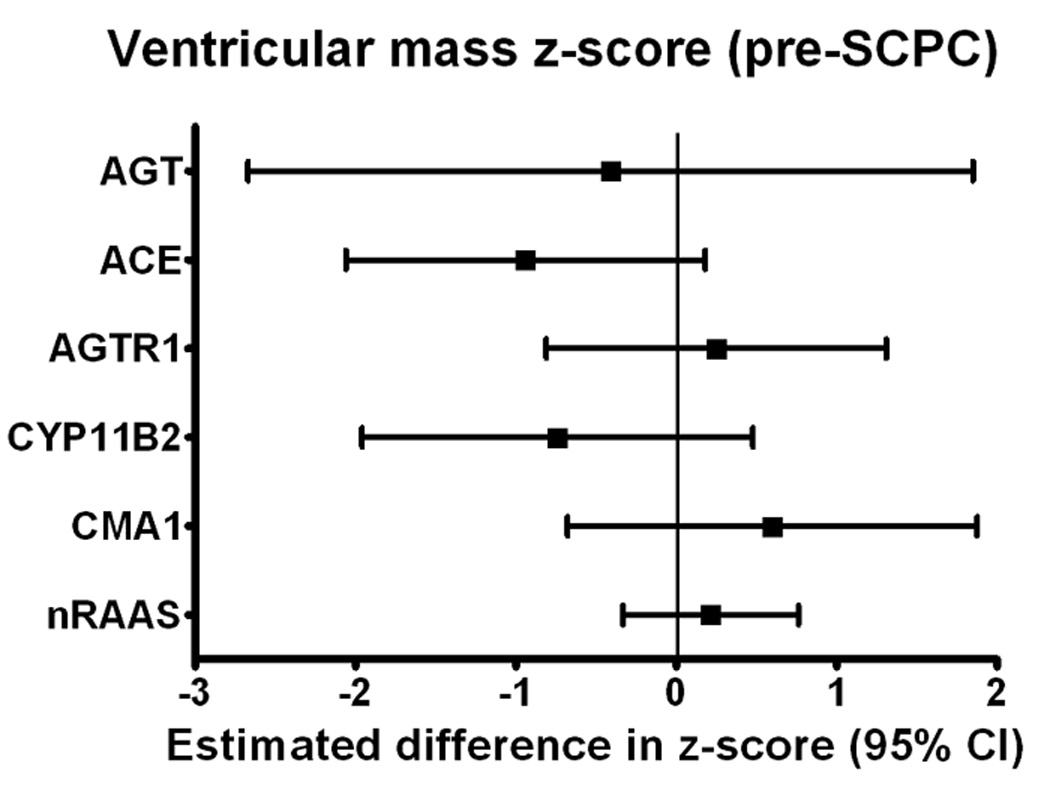
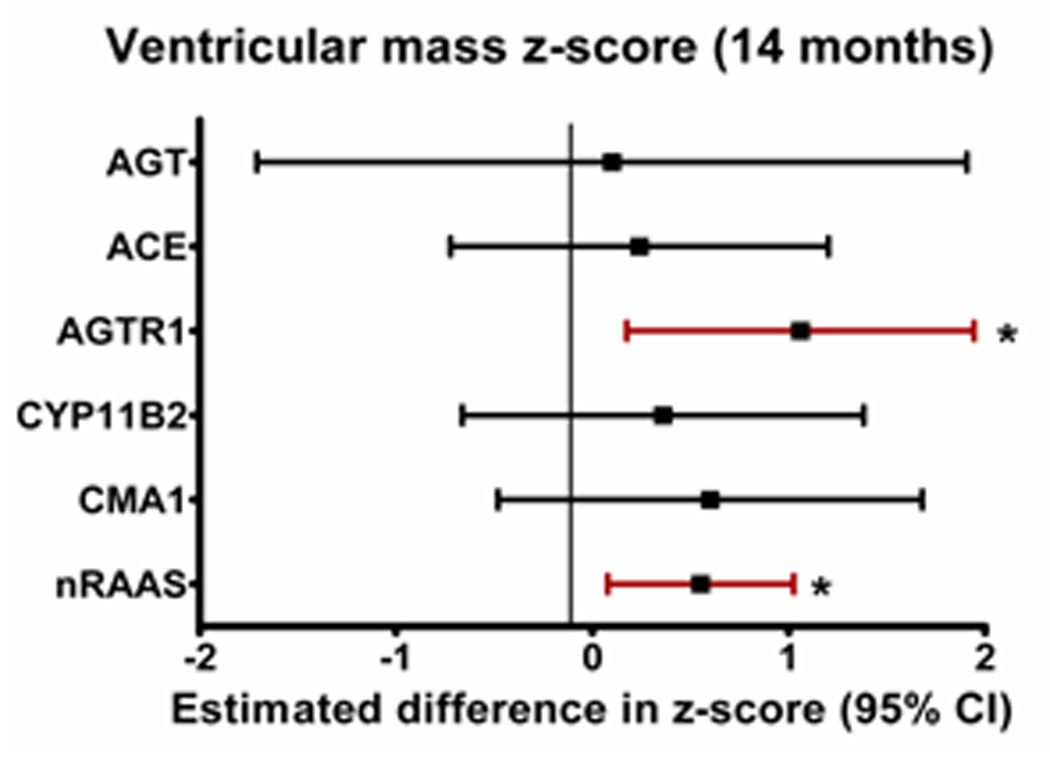
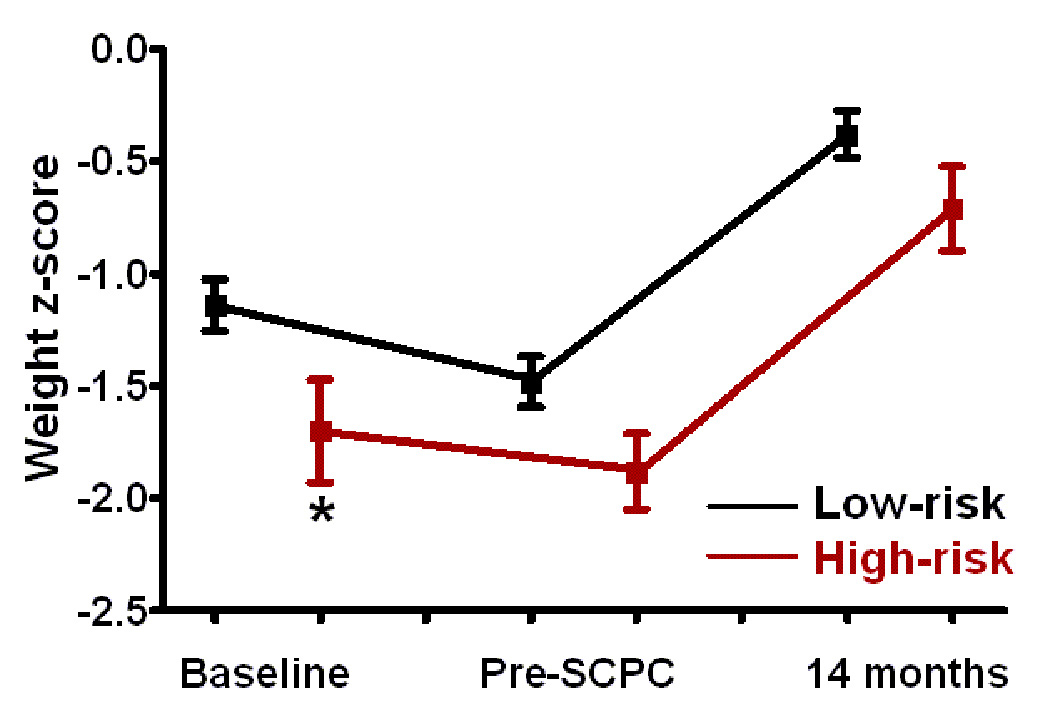
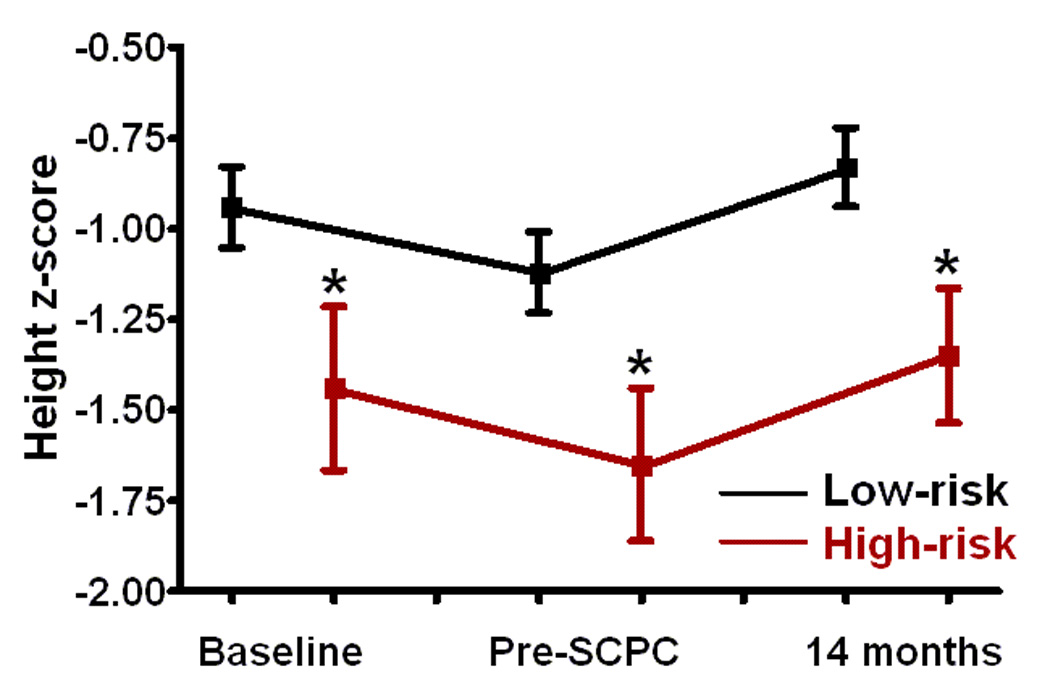
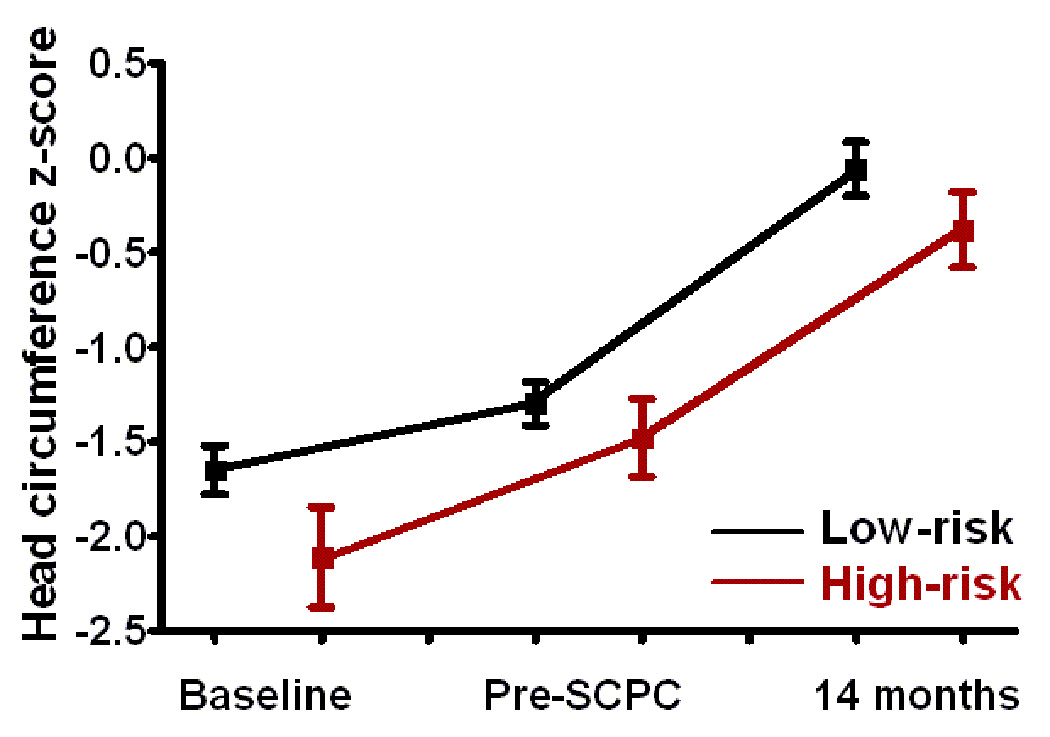
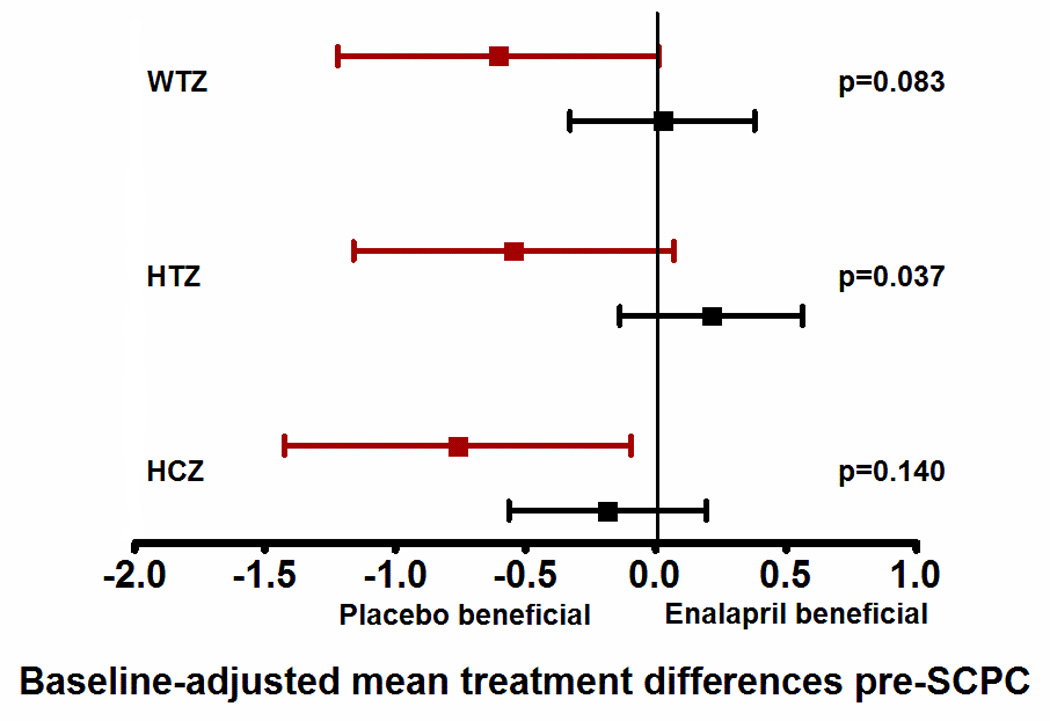
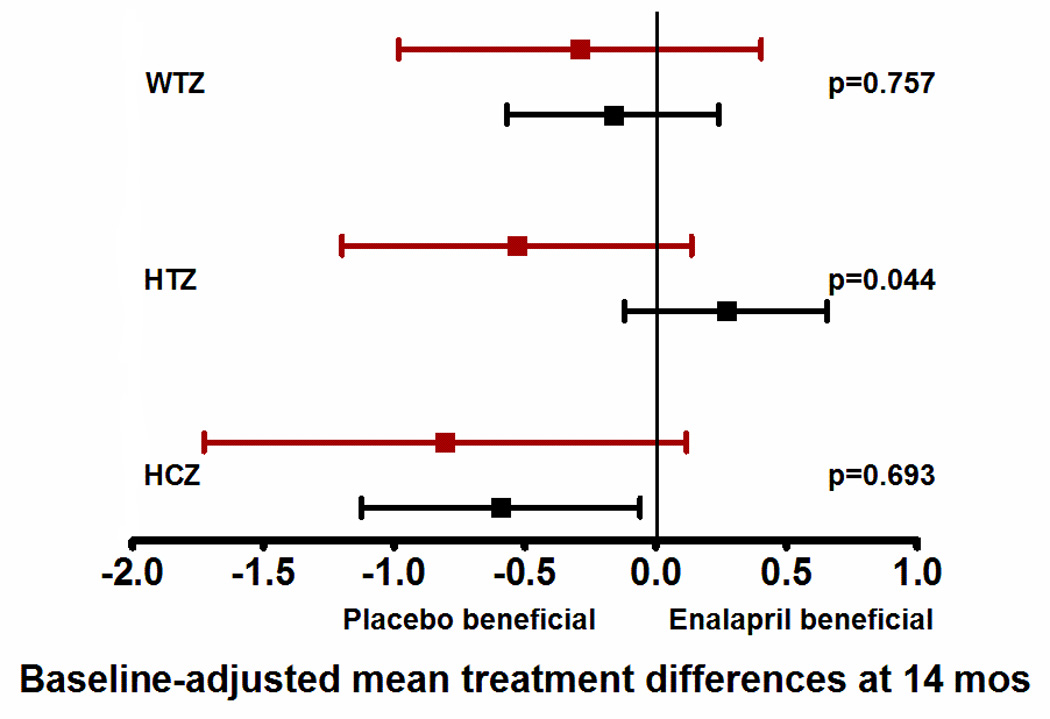
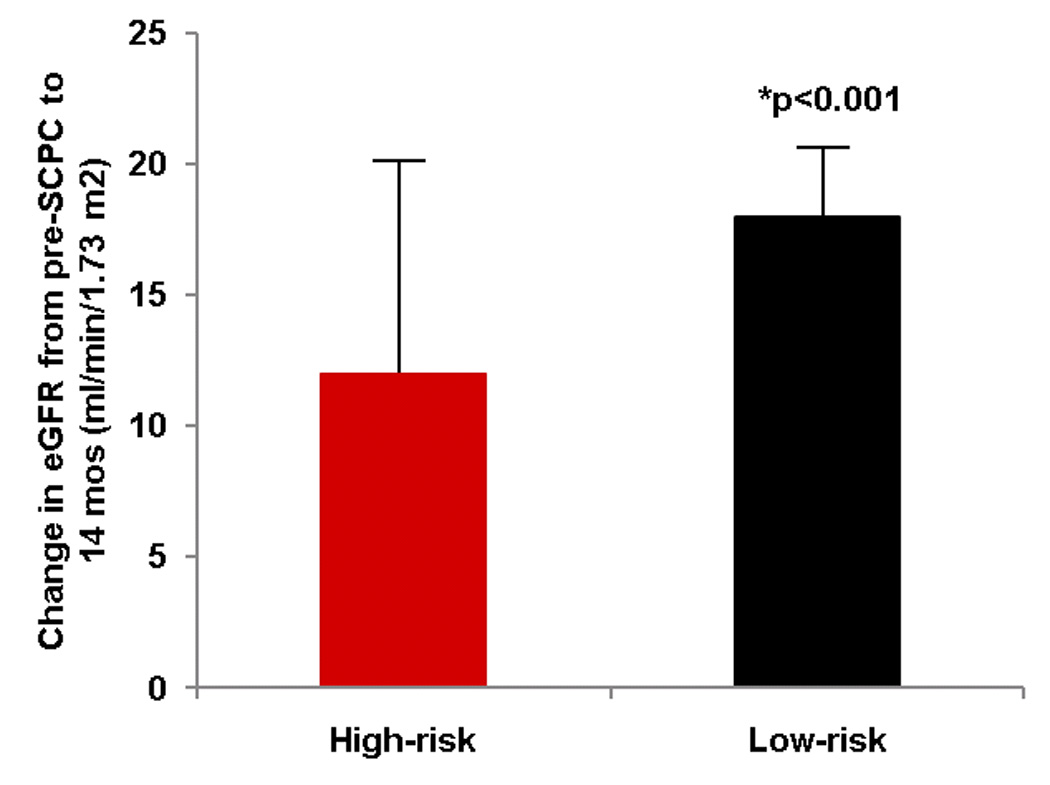
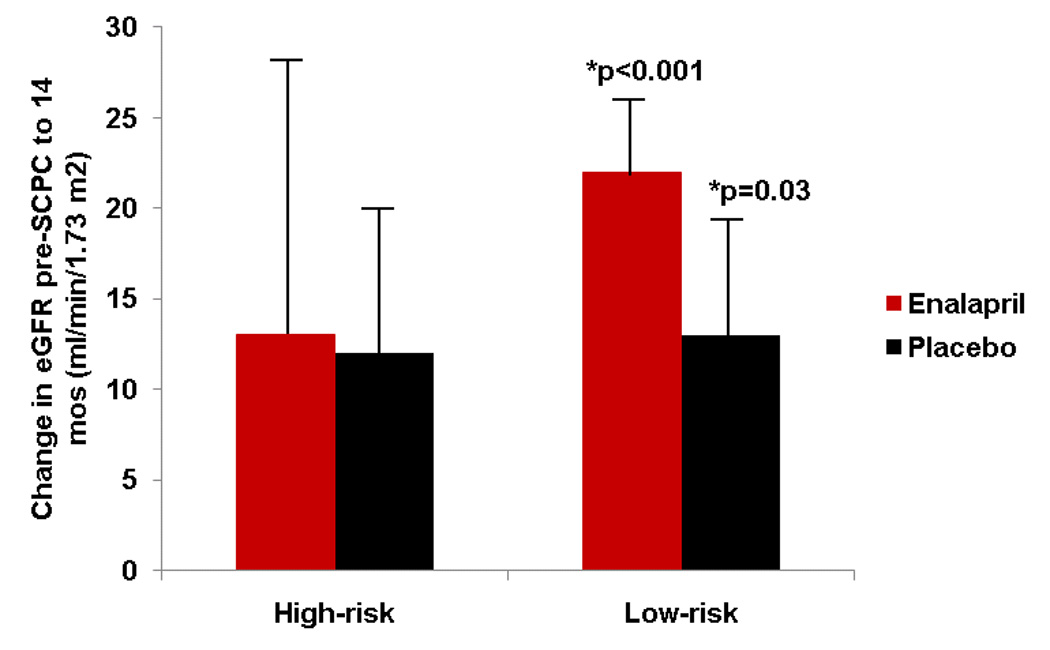
Methods and results: Single ventricle infants enrolled in a randomized trial of enalapril were genotyped for polymorphisms in 5 genes: angiotensinogen, angiotensin-converting enzyme, angiotensin II type 1 receptor, aldosterone synthase, and chymase. Alleles associated with renin-angiotensin-aldosterone system upregulation were classified as risk alleles. Ventricular mass, volume, somatic growth, renal function using estimated glomerular filtration rate, and response to enalapril were compared between patients with ≥2 homozygous risk genotypes (high risk), and those with <2 homozygous risk genotypes (low risk) at 2 time points: before the superior cavopulmonary connection (pre-SCPC) and at age 14 months. Of 230 trial subjects, 154 were genotyped: Thirty-eight were high risk, and 116 were low risk. Ventricular mass and volume were elevated in both groups pre-SCPC. Ventricular mass and volume decreased and estimated glomerular filtration rate increased after SCPC in the low-risk (P<0.05), but not the high-risk group. These responses were independent of enalapril treatment. Weight and height z-scores were lower at baseline, and height remained lower in the high-risk group at 14 months, especially in those receiving enalapril (P<0.05).
Conclusions: Renin-angiotensin-aldosterone system-upregulation genotypes were associated with failure of reverse remodeling after SCPC surgery, less improvement in renal function, and impaired somatic growth, the latter especially in patients receiving enalapril. Renin-angiotensin-aldosterone system genotype may identify a high-risk subgroup of single ventricle patients who fail to fully benefit from volume-unloading surgery. Follow-up is warranted to assess long-term impact.
Clinical trial registration: http://www.clinicaltrials.gov. Unique identifier: NCT00113087.
Figures
References
-
- Steinberger EK, Ferencz C, Loffredo CA. Infants with single ventricle: A population-based epidemiological study. Teratology. 2002;65:106–115. - PubMed
-
- Allgood NL, Alejos J, Drinkwater DC, Laks H, Williams RG. Effectiveness of the bidirectional glenn shunt procedure for volume unloading in the single ventricle patient. Am J Cardiol. 1994;74:834–836. - PubMed
-
- Gewillig MH, Lundstrom UR, Deanfield JE, Bull C, Franklin RC, Graham TP, Jr, Wyse RK. Impact of fontan operation on left ventricular size and contractility in tricuspid atresia. Circulation. 1990;81:118–127. - PubMed
-
- Gentles TL, Mayer JE, Jr, Gauvreau K, Newburger JW, Lock JE, Kupferschmid JP, Burnett J, Jonas RA, Castaneda AR, Wernovsky G. Fontan operation in five hundred consecutive patients: Factors influencing early and late outcome. J Thorac Cardiovasc Surg. 1997;114:376–391. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- HL068288/HL/NHLBI NIH HHS/United States
- HL068285/HL/NHLBI NIH HHS/United States
- U01 HL068269/HL/NHLBI NIH HHS/United States
- U01 HL068279/HL/NHLBI NIH HHS/United States
- U01 HL068290/HL/NHLBI NIH HHS/United States
- U10 HL068270/HL/NHLBI NIH HHS/United States
- U01 HL068281/HL/NHLBI NIH HHS/United States
- U01 HL085057/HL/NHLBI NIH HHS/United States
- HL068279/HL/NHLBI NIH HHS/United States
- U01 HL068288/HL/NHLBI NIH HHS/United States
- U01 HL068270/HL/NHLBI NIH HHS/United States
- HL085057/HL/NHLBI NIH HHS/United States
- HL068281/HL/NHLBI NIH HHS/United States
- U01 HL068292/HL/NHLBI NIH HHS/United States
- HL068269/HL/NHLBI NIH HHS/United States
- HL068270/HL/NHLBI NIH HHS/United States
- HL068290/HL/NHLBI NIH HHS/United States
- U10 HL109673/HL/NHLBI NIH HHS/United States
- U01 HL068285/HL/NHLBI NIH HHS/United States
- HL068292/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
