

Identifying the best therapy for chronic anal fissure
- PMID: 21577312
- PMCID: PMC3091162
- DOI: 10.4292/wjgpt.v2.i2.9
Identifying the best therapy for chronic anal fissure
Abstract
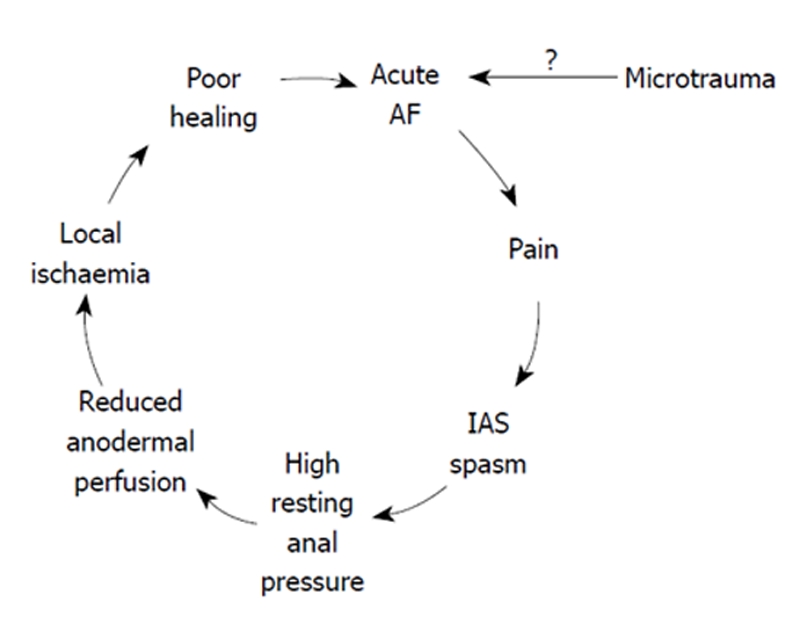
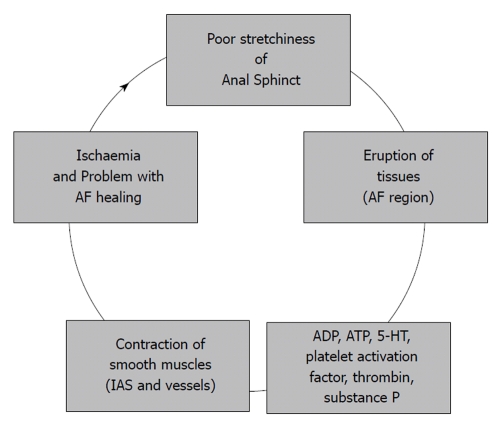
Chronic anal fissure (CAF) is a painful tear or crack which occurs in the anoderm. The optimal algorithm of therapy for CAF is still debated. Lateral internal sphincterotomy (LIS) is a surgical treatment, considered as the 'gold standard' therapy for CAF. It relieves CAF symptoms with a high rate of healing. Chemical sphincterotomy (CS) with nitrates, calcium blockers or botulinum toxin (BTX) is safe, with the rapid relief of pain, mild side-effects and no risk of surgery or anesthesia, but is a statistically less effective therapy for CAF than LIS. This article considers if aggressive treatment should only be offered to patients who fail pharmacological sphincterotomy. Aspects of anal fissure etiology, epidemiology and pathophysiology are considered with their meaning for further management of CAF. A molecular model of chemical interdependence significant for the chemistry of CAF healing is examined. Its application may influence the development of optimal therapy for CAF. BTX is currently considered the most effective type of CS and discussion in this article scrutinizes this method specifically. Although the effectiveness of BTX vs. LIS has been discussed, the essential focus of the article concerns identifying the best therapy application for anal fissure. Elements are presented which may help us to predict CAF healing. They provide rationale for the expansion of the CAF therapy algorithm. Ethical and economic factors are also considered in brief. As long as the patient is willing to accept the potential risk of fecal incontinence, we have grounds for the 'gold standard' (LIS) as the first-line treatment for CAF. The author concludes that, when the diagnosis of the anal fissure is established, CS should be considered for both ethical and economic reasons. He is convinced that a greater understanding and recognition of benign anal disorders by the GP and a proactive involvement at the point of initial diagnosis would facilitate the consideration of CS at an earlier, more practical stage with improved outcomes for the patient.
Keywords: Anal fissure; Benign anal diseases; Botulinum toxin; Chemical sphincterotomy; Ethics; Fissurectomy; Lateral internal sphincterotomy; Teaching.
Figures
References
-
- Dykes SL, Madoff RD. Benign Anorectal: Anal Fissure. In: Wolff BG, Fleshman JW, Beck DE, Pemberton JH, Wexner SD, et al., editors. The ASCRS textbook of colon and rectal surgery. New York: Springer Science and Business Media LLC; 2007. pp. 178–191.
-
- Aivaz O, Rayhanabad J, Nguyen V, Haigh PI, Abbas M. Botulinum toxin A with fissurectomy is a viable alternative to lateral internal sphincterotomy for chronic anal fissure. Am Surg. 2009;75:925–928. - PubMed
-
- Garcia-Aguilar J, Belmonte C, Wong WD, Lowry AC, Madoff RD. Open vs. closed sphincterotomy for chronic anal fissure: long-term results. Dis Colon Rectum. 1996;39:440–443. - PubMed
-
- Nyam DC, Pemberton JH. Long-term results of lateral internal sphincterotomy for chronic anal fissure with particular reference to incidence of fecal incontinence. Dis Colon Rectum. 1999;42:1306–1310. - PubMed
-
- Hyman N. Incontinence after lateral internal sphincterotomy: a prospective study and quality of life assessment. Dis Colon Rectum. 2004;47:35–38. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
