

Surgical trial in lobar intracerebral haemorrhage (STICH II) protocol
- PMID: 21586127
- PMCID: PMC3107158
- DOI: 10.1186/1745-6215-12-124
Surgical trial in lobar intracerebral haemorrhage (STICH II) protocol
Abstract
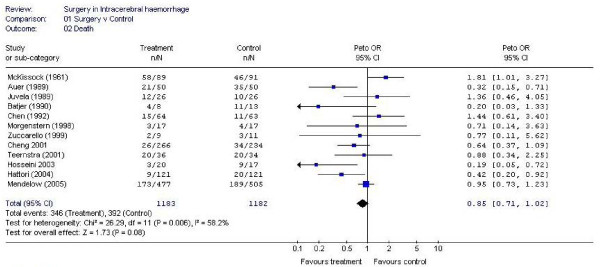
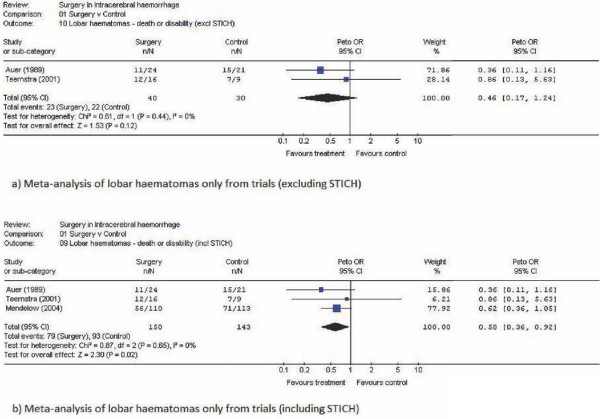
Background: Within the spectrum of spontaneous intracerebral haemorrhage there are some patients with large or space occupying haemorrhage who require surgery for neurological deterioration and others with small haematomas who should be managed conservatively. There is equipoise about the management of patients between these two extremes. In particular there is some evidence that patients with lobar haematomas and no intraventricular haemorrhage might benefit from haematoma evacuation. The STICH II study will establish whether a policy of earlier surgical evacuation of the haematoma in selected patients will improve outcome compared to a policy of initial conservative treatment.
Methods/design: An international multicentre randomised parallel group trial. Only patients for whom the treating neurosurgeon is in equipoise about the benefits of early craniotomy compared to initial conservative treatment are eligible. All patients must have a CT scan confirming spontaneous lobar intracerebral haemorrhage (≤1 cm from the cortex surface of the brain and 10-100 ml in volume). Any clotting or coagulation problems must be corrected and randomisation must take place within 48 hours of ictus. With 600 patients, the study will be able to demonstrate a 12% benefit from surgery (2p < 0.05) with 80% power.Stratified randomisation is undertaken using a central 24 hour randomisation service accessed by telephone or web. Patients randomised to early surgery should have the operation within 12 hours. Information about the status (Glasgow Coma Score and focal signs) of all patients through the first five days of their trial progress is also collected in addition to another CT scan at about five days (+/- 2 days). Outcome is measured at six months via a postal questionnaire to the patient. Primary outcome is death or severe disability defined using a prognosis based 8 point Glasgow Outcome Scale. Secondary outcomes include: Mortality, Rankin, Barthel, EuroQol, and Survival.
Trial registration: ISRCTN: ISRCTN22153967.
© 2011 Mendelow et al; licensee BioMed Central Ltd.
Figures
References
-
- Bamford J, Sandercock P, Dennis M, Burn J, Warlow C. A prospective-study of acute cerebrovascular disease in the community - the Oxfordshire Community Stroke Project 1981-86.2. Incidence, case fatality rates and overall outcome at one year of cerebral infarction, primary intracerebral and subarachnoid hemorrhage. Journal Of Neurology Neurosurgery And Psychiatry. 1990;53(1):16–22. doi: 10.1136/jnnp.53.1.16. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
