

Malignant tumours of the small intestine: a review of histopathology, multidetector CT and MRI aspects
- PMID: 21586504
- PMCID: PMC3473441
- DOI: 10.1259/bjr/20673379
Malignant tumours of the small intestine: a review of histopathology, multidetector CT and MRI aspects
Abstract
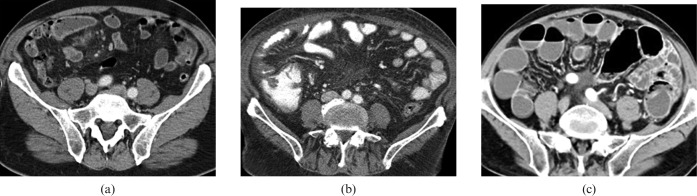
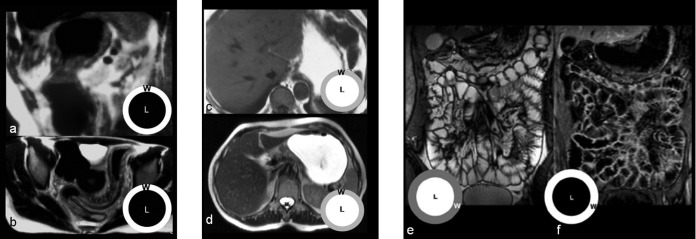
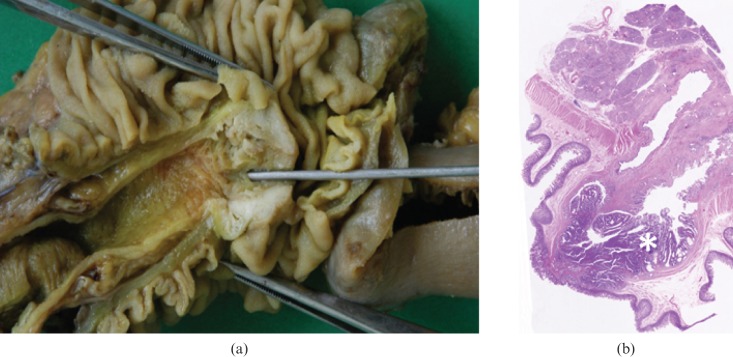
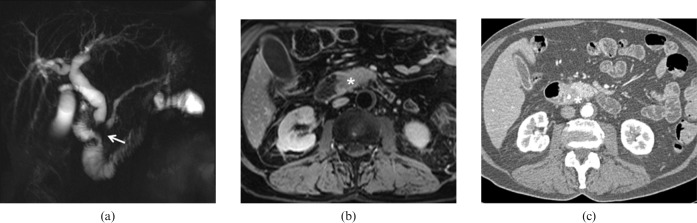
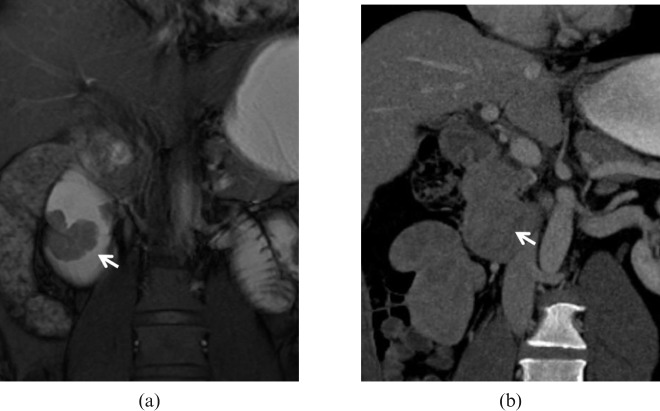
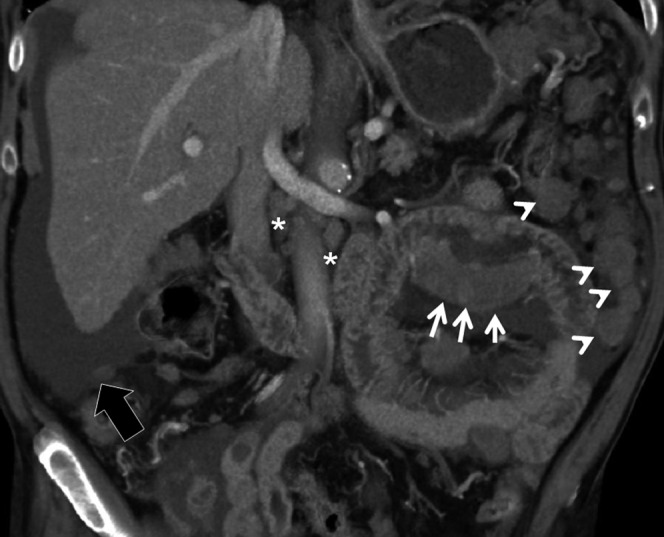
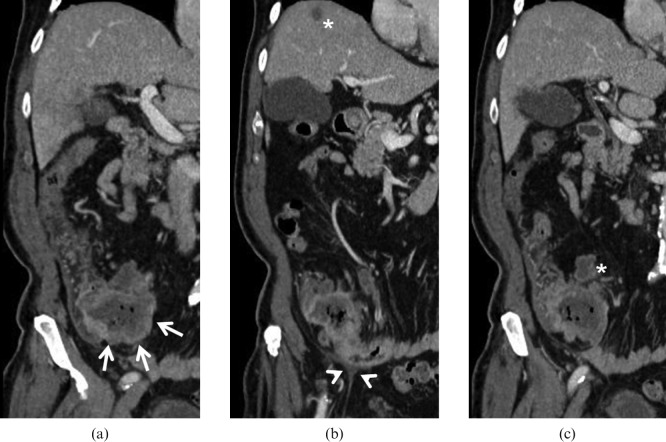
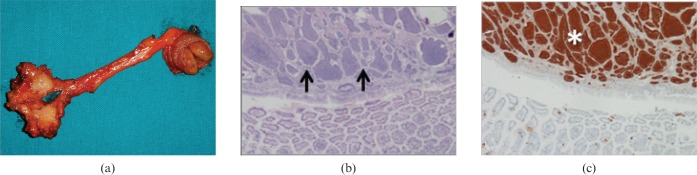
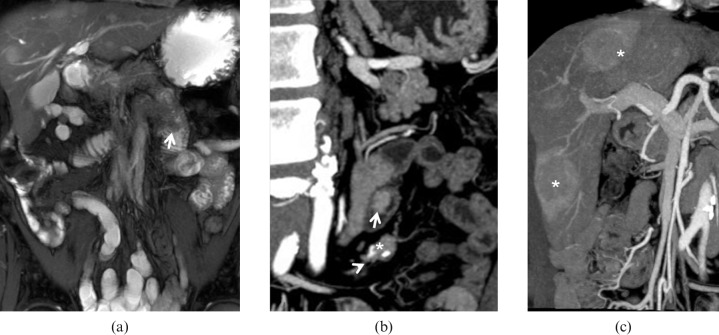
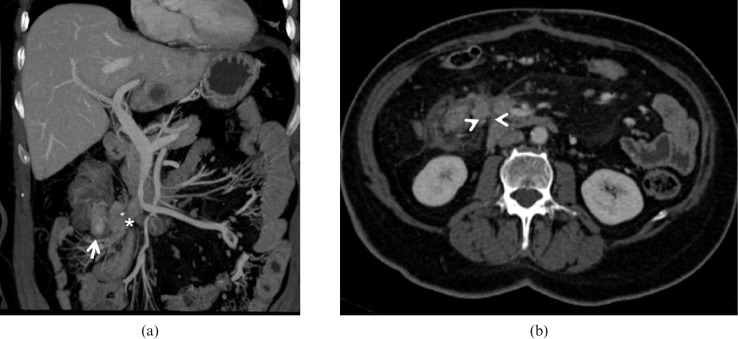
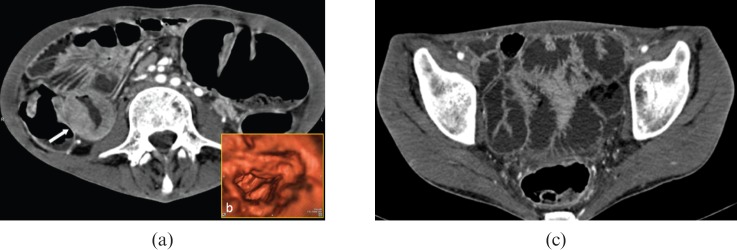
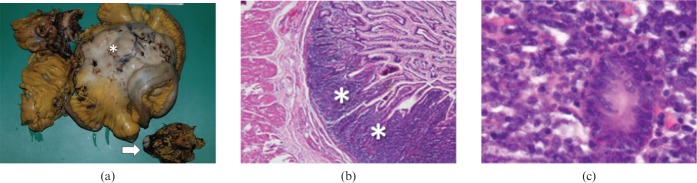
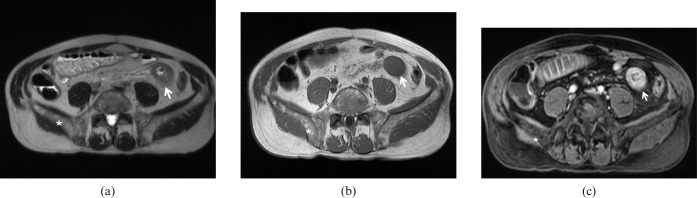
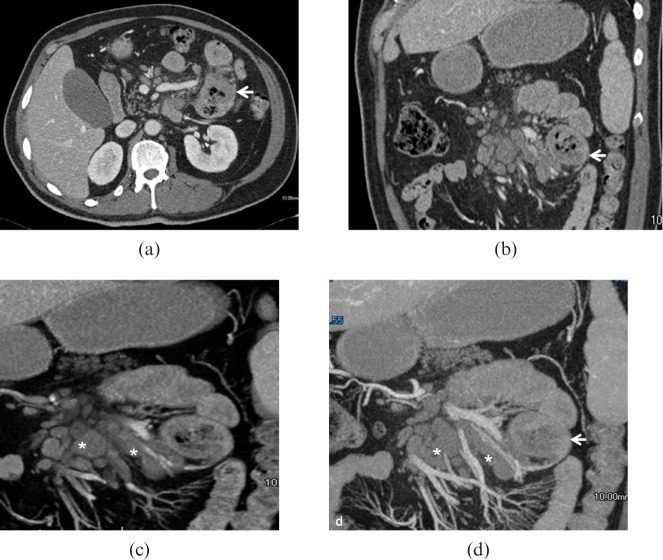
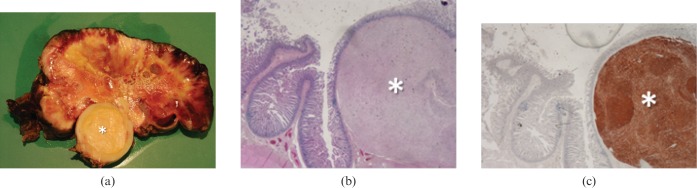
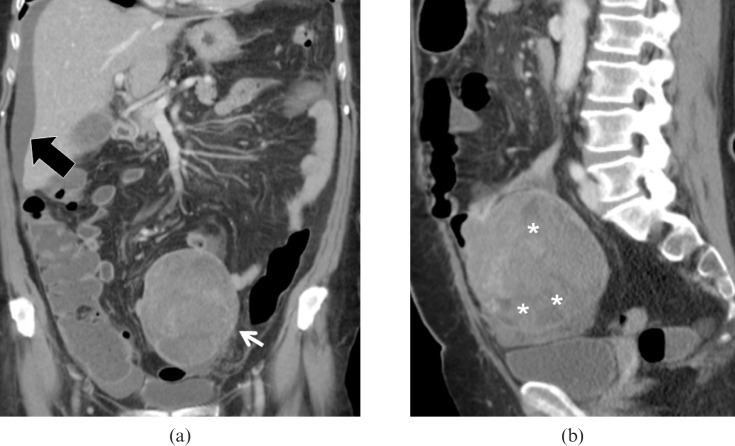
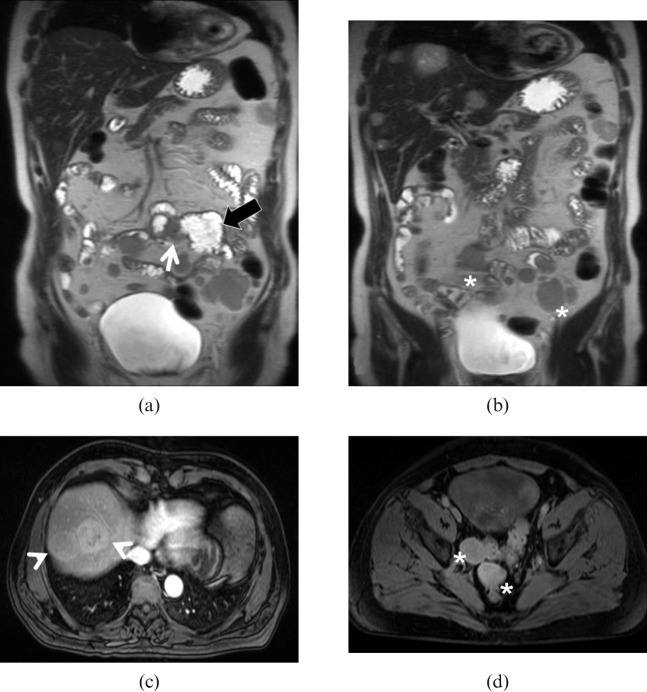
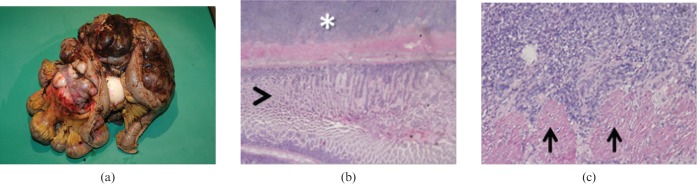
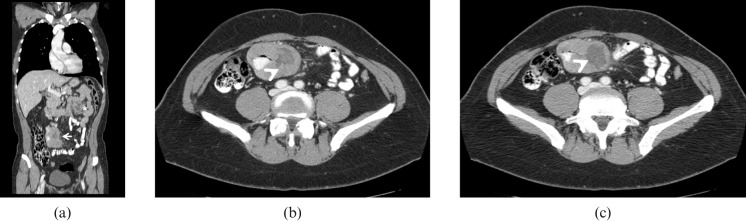
Small bowel neoplasms, including adenocarcinoma, carcinoid tumour, lymphoma and gastrointestinal stromal tumours, represent a small percentage of gastrointestinal cancers, yet are among those with the poorest prognosis compared with other gastrointestinal malignancies. Unclear clinical scenarios and difficult radiological diagnosis often delay treatment with negative effects on patient survival. Recently, multidetector CT (MDCT) and MRI have been introduced as feasible and accurate diagnostic techniques for the identification and staging of small bowel neoplasms. These techniques are gradually replacing conventional barium radiography as the tool of choice. However, the inherent technical and physiological challenges of small bowel imaging require a familiarity with patient preparation and scan protocols. Adequate knowledge of the histopathology and natural evolution of small bowel neoplasms is also important for differential diagnosis. The aim of this article is to review MDCT and MRI protocols for the evaluation of small bowel tumours and to provide a concise yet comprehensive guide to the most relevant imaging features relative to histopathology.
Figures
References
-
- Martin RG. Malignant tumors of the small intestine. Surg Clin North Am 1986;66:779–85 - PubMed
-
- North JH, Pack MS. Malignant tumors of the small intestine: a review of 144 cases. Am Surg 2000;66:46–51 - PubMed
-
- Horner MJ, Ries LAG, Krapcho M, Neyman N, Aminou R, Howlader N, et al., editors. SEER cancer statistics review, 1975-2006, National Cancer Institute: Bethesda, MD. Available at: http://seer.cancer.gov/csr/1975_2006/
-
- Yamagami H, Oshitani N, Hosomi S, Suekane T, Kamata N, Sogawa M, et al. Usefulness of double-balloon endoscopy in the diagnosis of malignant small-bowel tumors. Clin Gastroenterol Hepatol 2008;6:1202–5 - PubMed
-
- Maglinte DD, O'Connor K, Bessette J, Chernish SM, Kelvin FM. The role of the physician in the late diagnosis of primary malignant tumors of the small intestine. Am J Gastroenterol 1991;86:304–8 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
