

Factors associated with closures of emergency departments in the United States
- PMID: 21586713
- PMCID: PMC4063529
- DOI: 10.1001/jama.2011.620
Factors associated with closures of emergency departments in the United States
Erratum in
- JAMA. 2011 Jul 13;306(2):162
Abstract
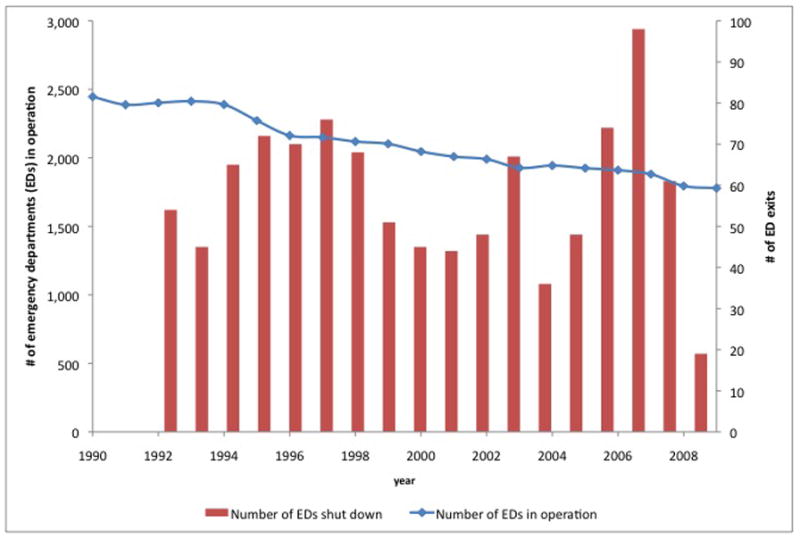
Context: Between 1998 and 2008, the number of hospital-based emergency departments (EDs) in the United States declined, while the number of ED visits increased, particularly visits by patients who were publicly insured and uninsured. Little is known about the hospital, community, and market factors associated with ED closures. Federal law requiring EDs to treat all in need regardless of a patient's ability to pay may make EDs more vulnerable to the market forces that govern US health care.
Objective: To determine hospital, community, and market factors associated with ED closures.
Design: Emergency department and hospital organizational information from 1990 through 2009 was acquired from the American Hospital Association (AHA) Annual Surveys (annual response rates ranging from 84%-92%) and merged with hospital financial and payer mix information available through 2007 from Medicare hospital cost reports. We evaluated 3 sets of risk factors: hospital characteristics (safety net [as defined by hospitals caring for more than double their Medicaid share of discharges compared with other hospitals within a 15-mile radius], ownership, teaching status, system membership, ED size, case mix), county population demographics (race, poverty, uninsurance, elderly), and market factors (ownership mix, profit margin, location in a competitive market, presence of other EDs).
Setting: All general, acute, nonrural, short-stay hospitals in the United States with an operating ED anytime from 1990-2009.
Main outcome measure: Closure of an ED during the study period.
Results: From 1990 to 2009, the number of hospitals with EDs in nonrural areas declined from 2446 to 1779, with 1041 EDs closing and 374 hospitals opening EDs. Based on analysis of 2814 urban acute-care hospitals, constituting 36,335 hospital-year observations over an 18-year study interval (1990-2007), for-profit hospitals and those with low profit margins were more likely to close than their counterparts (cumulative hazard rate based on bivariate model, 26% vs 16%; hazard ratio [HR], 1.8; 95% confidence interval [CI], 1.5-2.1, and 36% vs 18%; HR, 1.9; 95% CI, 1.6-2.3, respectively). Hospitals in more competitive markets had a significantly higher risk of closing their EDs (34% vs 17%; HR, 1.3; 95% CI, 1.1-1.6), as did safety-net hospitals (10% vs 6%; HR, 1.4; 95% CI, 1.1-1.7) and those serving a higher share of populations in poverty (37% vs 31%; HR, 1.4; 95% CI, 1.1-1.7).
Conclusion: From 1990 to 2009, the number of hospital EDs in nonrural areas declined by 27%, with for-profit ownership, location in a competitive market, safety-net status, and low profit margin associated with increased risk of ED closure.
Conflict of interest statement
All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest and none were reported.
Figures


Comment in
-
Emergency department closures in the United States.JAMA. 2011 Sep 7;306(9):929; author reply 929-30. doi: 10.1001/jama.2011.1257. JAMA. 2011. PMID: 21900129 No abstract available.
References
-
- Institute of Medicine. Hospital-Based Emergency Care: At the Breaking Point. Paper presented at: Institute of Medicine; 2007; Washington, DC. 2007.
-
-
Emergency Medical Treatment and Active Labor Act, 42 USC §1395dd (2000).
-
-
- Pitts SR, Carrier ER, Rich EC, Kellermann AL. Where Americans get acute care: increasingly, it’s not at their doctor’s office. Health affairs (Project Hope) 2010 Sep;29(9):1620–1629. - PubMed
-
-
Sec. 10101, and Section 3504, Patient Protection and Affordable Care Act of 2010, Pub.L. 111–148, 124 Stat. 119, to be codified as amended at scattered sections of 42 U.S.C.
-
-
- American Hospital Association. [Accessed March 29, 2011];Trendwatch Chartbook 2010: Trends Affecting Hospitals and Health Systems. 2010 Appendix 3, Table 3.3. http://www.aha.org/aha/research-and-trends/chartbook/2010chartbook.html.
