

Accuracy of relocation, evaluation of geometric uncertainties and clinical target volume (CTV) to planning target volume (PTV) margin in fractionated stereotactic radiotherapy for intracranial tumors using relocatable Gill-Thomas-Cosman (GTC) frame
- PMID: 21587166
- PMCID: PMC5718666
- DOI: 10.1120/jacmp.v12i2.3260
Accuracy of relocation, evaluation of geometric uncertainties and clinical target volume (CTV) to planning target volume (PTV) margin in fractionated stereotactic radiotherapy for intracranial tumors using relocatable Gill-Thomas-Cosman (GTC) frame
Abstract
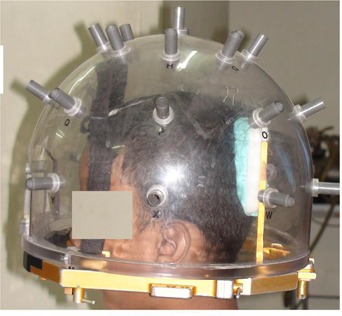
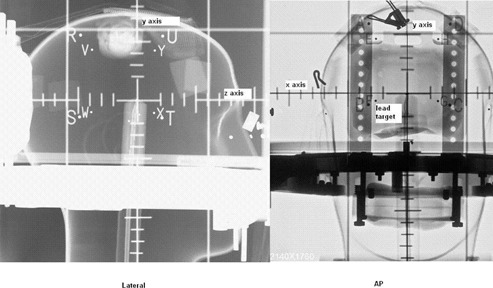
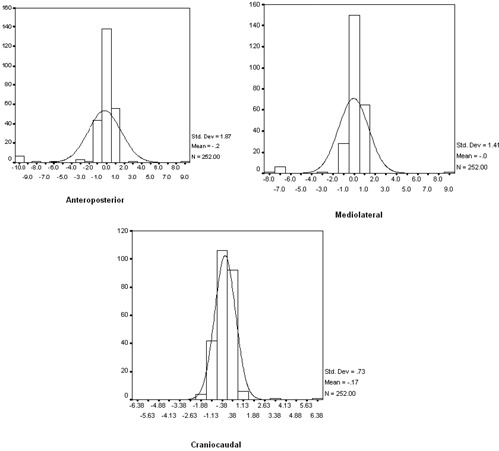
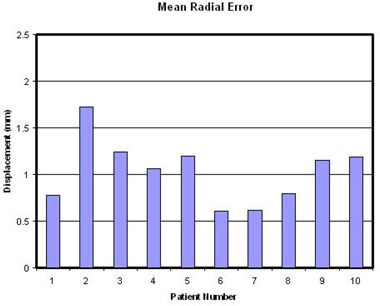
The present study is aimed at determination of accuracy of relocation of Gill-Thomas-Cosman frame during fractionated stereotactic radiotherapy. The study aims to quantitatively determine the magnitudes of error in anteroposterior, mediolateral and craniocaudal directions, and determine the margin between clinical target volume to planning target volume based on systematic and random errors. Daily relocation error was measured using depth helmet and measuring probe. Based on the measurements, translational displacements in anteroposterior (z), mediolateral (x), and craniocaudal (y) directions were calculated. Based on the displacements in x, y and z directions, systematic and random error were calculated and three-dimensional radial displacement vector was determined. Systematic and random errors were used to derive CTV to PTV margin. The errors were within ± 2 mm in 99.2% cases in anteroposterior direction (AP), in 99.6% cases in mediolateral direction (ML), and in 97.6% cases in craniocaudal direction (CC). In AP, ML and CC directions, systematic errors were 0.56, 0.38, 0.42 mm and random errors were 1.86, 1.36 and 0.73 mm, respectively. Mean radial displacement was 1.03 mm ± 0.34. CTV to PTV margins calculated by ICRU formula were 1.86, 1.45 and 0.93 mm; by Stroom's formula they were 2.42, 1.74 and 1.35 mm; by van Herk's formula they were 2.7, 1.93 and 1.56 mm (AP, ML and CC directions). Depth helmet with measuring probe provides a clinically viable way for assessing the relocation accuracy of GTC frame. The errors were within ± 2 mm in all directions. Systematic and random errors were more along the anteroposterior axes. According to the ICRU formula, a margin of 2 mm around the tumor seems to be adequate.
Figures
References
-
- Burton KE, Thomas SJ, Whitney D, Routsis DS, Benson RJ, Burnet NG. Accuracy of a relocatable stereotactic radiotherapy head frame evaluated by use of a depth helmet. Clin Oncol. 2002;14(1):31–39. - PubMed
-
- Schlegel W, Pastyr O, Bortfeld T, Gademann G, Menke M, Maier‐Borst W. Stereotactically guided fractionated radiotherapy: technical aspects. Radiother Oncol. 1993;29(2):197–204. - PubMed
-
- Hamilton RJ, Kuchnir FT, Pelizzari CA, Sweeney PJ, Rubin SJ. Repositioning accuracy of a noninvasive head fixation system for stereotactic radiotherapy. Med Phys. 1996;23(11):1909–17. - PubMed
-
- Bednartz G. Interim report of a randomized trial comparing two forms of immobilization of the head for fractionated stereotactic radiotherapy [abstract]. Proceedings of the 48th Annual ASTRO Meeting; 2006 Nov. 5–9; Philadelphia, PA. Fairfax, VA: ASTRO; 2006. - PubMed
-
- Jaywant S. Immobilization in stereotactic radiotherapy: radionics GTC versus HNL [abstract]. Proceedings of the 48th Annual ASTRO Meeting; 2006 Nov. 5–9; Philadelphia, PA. Fairfax, VA: ASTRO; 2006.
MeSH terms
LinkOut - more resources
Full Text Sources
