

Viable tumor tissue adherent to needle applicators after local ablation: a risk factor for local tumor progression
- PMID: 21590455
- PMCID: PMC3222809
- DOI: 10.1245/s10434-011-1762-8
Viable tumor tissue adherent to needle applicators after local ablation: a risk factor for local tumor progression
Abstract
Background: Local tumor progression (LTP) is a serious complication after local ablation of malignant liver tumors, negatively influencing patient survival. LTP may be the result of incomplete ablation of the treated tumor. In this study, we determined whether viable tumor cells attached to the needle applicator after ablation was associated with LTP and disease-free survival.
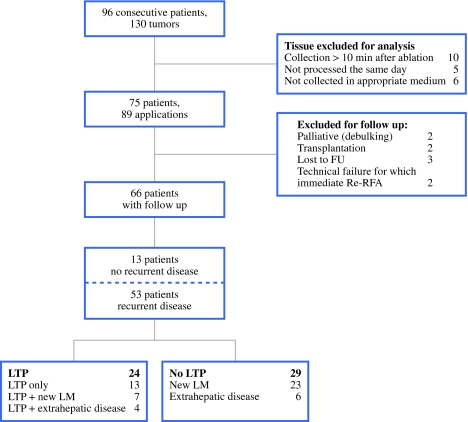
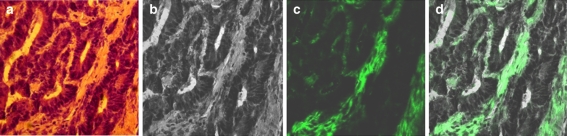
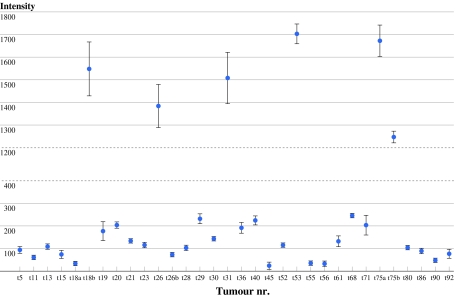
Methods: In this prospective study, tissue was collected of 96 consecutive patients who underwent local liver ablations for 130 liver malignancies. Cells and tissue attached to the needle applicators were analyzed for viability using glucose-6-phosphate-dehydrogenase staining and autofluorescence intensity levels of H&E stained sections. Patients were followed-up until disease progression.
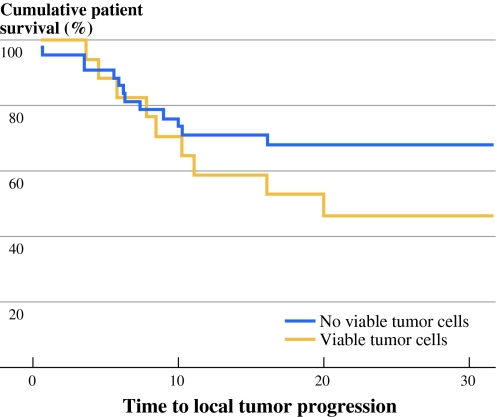
Results: Viable tumor cells were found on the needle applicators after local ablation in 26.7% of patients. The type of needle applicator used, an open approach, and the omission of track ablation were significantly correlated with viable tumor tissue adherent to the needle applicator. The presence of viable cells was an independent predictor of LTP. The attachment of viable cells to the needle applicators was associated with a shorter time to LTP.
Conclusions: Viable tumor cells adherent to the needle applicators were found after ablation of 26.7% of patients. An independent risk factor for viable cells adherent to the needle applicators is the omission of track ablation. We recommend using only RFA devices that have track ablation functionality. Adherence of viable tumor cells to the needle applicator after local ablation was an independent risk factor for LTP.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
