

Acute HIV-1 Infection
- PMID: 21591946
- PMCID: PMC3771113
- DOI: 10.1056/NEJMra1011874
Acute HIV-1 Infection
Abstract
In 2009, the United Nations Estimated that 33.2 Million People worldwide were living with human immunodeficiency virus type 1 (HIV-1) infection and that 2.6 million people had been newly infected. The need for effective HIV-1 prevention has never been greater. In this review, we address recent critical advances in our understanding of HIV-1 transmission and acute HIV-1 infection. Fourth-generation HIV-1 testing, now available worldwide,, will allow the diagnosis of infection in many patients and may lead to new treatments and opportunities for prevention.
Conflict of interest statement
Dr. Cohen reports receiving consulting fees from GlaxoSmith-Kline and Merck; Dr. McMichael, receiving payment for the development of educational presentations from Henry Stewart Talks; and Dr. Haynes, receiving a research grant from Peregrine Pharmaceuticals. No other potential conflict of interest relevant to this article was reported.
Figures
References
-
- Global report 2010. Geneva: UNAIDS; 2010. http://www.unaids.org/globalreport/documents/20101123_GlobalReport_full_....
-
- Branson BM. State of the art for diagnosis of HIV infection. Clin Infect Dis. 2007;45(Suppl 4):S221–S225. - PubMed
-
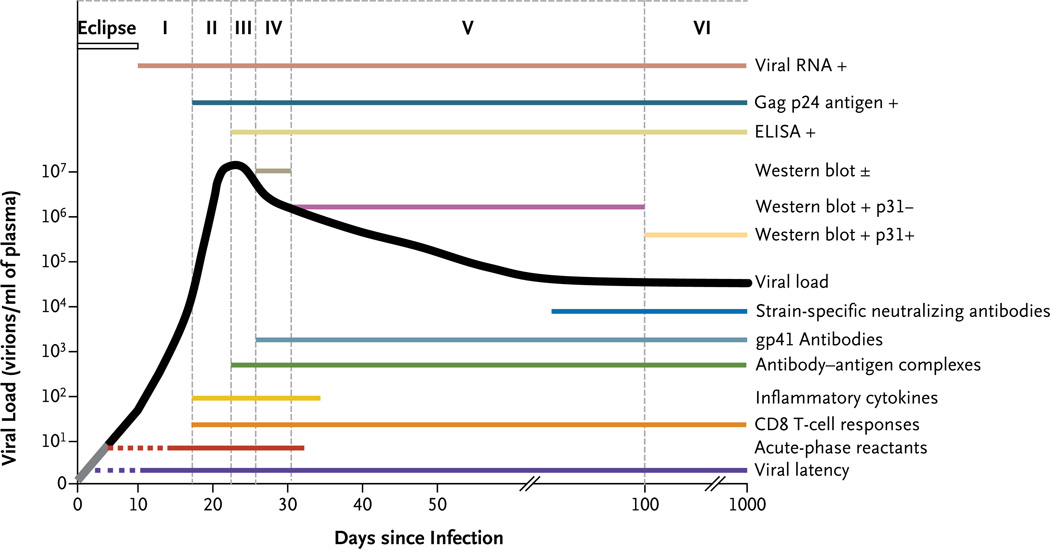
- Fiebig EW, Wright DJ, Rawal BD, et al. Dynamics of HIV viremia and antibody seroconversion in plasma donors: implications for diagnosis and staging of primary HIV infection. AIDS. 2003;17:1871–1879. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical