

Association between a quantitative CT scan measure of brain edema and outcome after cardiac arrest
- PMID: 21592642
- PMCID: PMC3244968
- DOI: 10.1016/j.resuscitation.2011.04.001
Association between a quantitative CT scan measure of brain edema and outcome after cardiac arrest
Abstract
Background: Cerebral edema is one physical change associated with brain injury and decreased survival after cardiac arrest. Edema appears on computed tomography (CT) scan of the brain as decreased X-ray attenuation by gray matter. This study tested whether the gray matter attenuation to white matter attenuation ratio (GWR) was associated with survival and functional recovery.
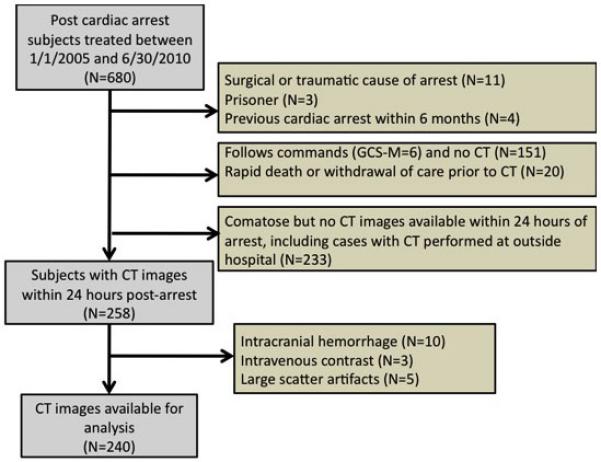
Methods: Subjects were patients hospitalized after cardiac arrest at a single institution between 1/1/2005 and 7/30/2010. Subjects were included if they had non-traumatic cardiac arrest and a non-contrast CT scan within 24h after cardiac arrest. Attenuation (Hounsfield Units) was measured in gray matter (caudate nucleus, putamen, thalamus, and cortex) and in white matter (internal capsule, corpus callosum and centrum semiovale). The GWR was calculated for basal ganglia and cerebrum. Outcomes included survival and functional status at hospital discharge.
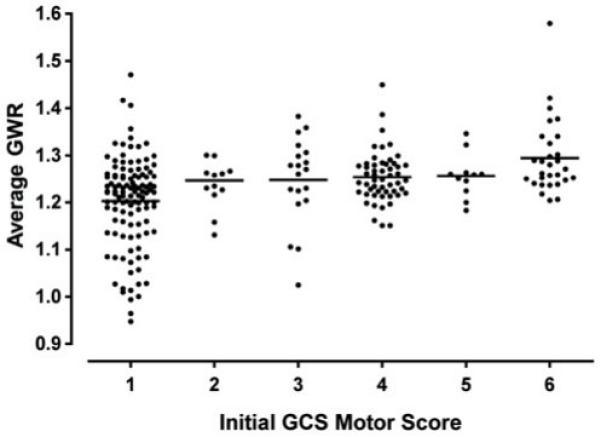
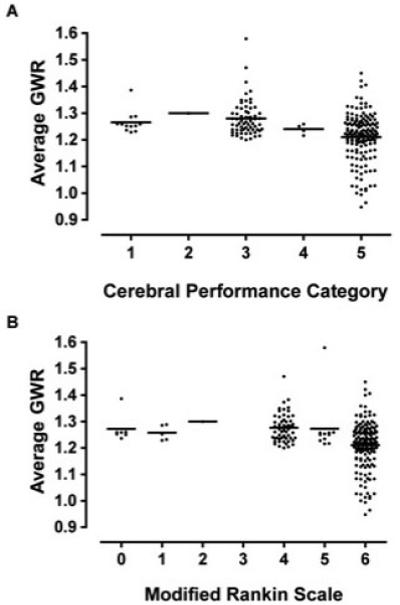
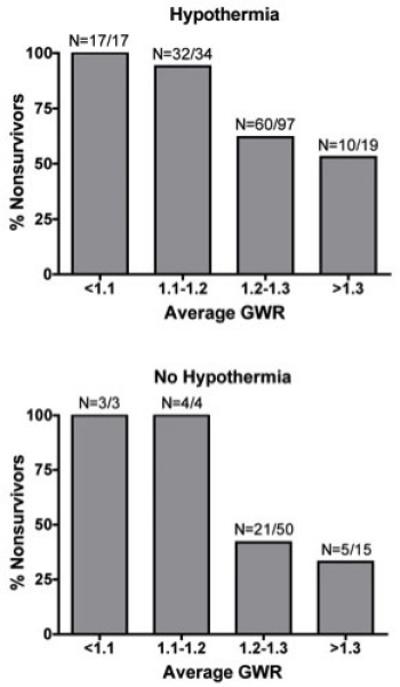
Results: For 680 patients, 258 CT scans were available, but 18 were excluded because of hemorrhage (10), intravenous contrast (3) or technical artifact (5), leaving 240 CT scans for analysis. Lower GWR values were associated with lower initial Glasgow Coma Scale motor score. Overall survival was 36%, but decreased with decreasing GWR. The average of basal ganglia and cerebrum GWR provided the best discrimination. Only 2/58 subjects with average GWR<1.20 survived and both were treated with hypothermia. The association of GWR with functional outcome was completely explained by mortality when GWR<1.20.
Conclusions: Subjects with severe cerebral edema, defined by GWR<1.20, have very low survival with conventional care, including hypothermia. GWR estimates pre-treatment likelihood of survival after cardiac arrest.
Copyright © 2011 Elsevier Ireland Ltd. All rights reserved.
Figures
Comment in
-
Imaging brain injury after cardiac arrest resuscitation when it really matters.Resuscitation. 2011 Sep;82(9):1124-5. doi: 10.1016/j.resuscitation.2011.05.029. Epub 2011 Jun 14. Resuscitation. 2011. PMID: 21719185 No abstract available.
Similar articles
-
Time-dependent association of grey-white ratio on early brain CT predicting outcomes after cardiac arrest at hospital discharge.Resuscitation. 2025 Jan;206:110440. doi: 10.1016/j.resuscitation.2024.110440. Epub 2024 Nov 26. Resuscitation. 2025. PMID: 39592066
-
The association between a quantitative computed tomography (CT) measurement of cerebral edema and outcomes in post-cardiac arrest-a validation study.Resuscitation. 2014 Oct;85(10):1348-53. doi: 10.1016/j.resuscitation.2014.05.022. Epub 2014 Jun 2. Resuscitation. 2014. PMID: 24892267 Free PMC article.
-
[Neurological prognostic value of gray-white-matter ratio in patients after respiratory and cardiac arrest].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017 Oct;29(10):893-896. doi: 10.3760/cma.j.issn.2095-4352.2017.10.006. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017. PMID: 29017648 Chinese.
-
Gray matter to white matter ratio for predicting neurological outcomes in patients treated with target temperature management after cardiac arrest: A systematic review and meta-analysis.Resuscitation. 2018 Nov;132:21-28. doi: 10.1016/j.resuscitation.2018.08.024. Epub 2018 Aug 27. Resuscitation. 2018. PMID: 30165096
-
Prognostic Values of the Gray-to-White Matter Ratio on Brain Computed Tomography Images for Neurological Outcomes after Cardiac Arrest: A Meta-Analysis.Biomed Res Int. 2020 Nov 3;2020:7949516. doi: 10.1155/2020/7949516. eCollection 2020. Biomed Res Int. 2020. PMID: 33490256 Free PMC article.
Cited by
-
Are providers overconfident in predicting outcome after cardiac arrest?Resuscitation. 2020 Aug;153:97-104. doi: 10.1016/j.resuscitation.2020.06.004. Epub 2020 Jun 13. Resuscitation. 2020. PMID: 32544415 Free PMC article.
-
Recovery among post-arrest patients with mild-to-moderate cerebral edema.Resuscitation. 2021 May;162:149-153. doi: 10.1016/j.resuscitation.2021.02.033. Epub 2021 Mar 1. Resuscitation. 2021. PMID: 33662524 Free PMC article.
-
Lipidomics Detection of Brain Cardiolipins in Plasma Is Associated With Outcome After Cardiac Arrest.Crit Care Med. 2019 Apr;47(4):e292-e300. doi: 10.1097/CCM.0000000000003636. Crit Care Med. 2019. PMID: 30855329 Free PMC article.
-
Effect of neuromonitor-guided titrated care on brain tissue hypoxia after opioid overdose cardiac arrest.Resuscitation. 2018 Aug;129:121-126. doi: 10.1016/j.resuscitation.2018.04.013. Epub 2018 Apr 18. Resuscitation. 2018. PMID: 29679696 Free PMC article.
-
Standardised and automated assessment of head computed tomography reliably predicts poor functional outcome after cardiac arrest: a prospective multicentre study.Intensive Care Med. 2024 Jul;50(7):1096-1107. doi: 10.1007/s00134-024-07497-2. Epub 2024 Jun 20. Intensive Care Med. 2024. PMID: 38900283 Free PMC article.
References
-
- Neumar RW, Nolan JP, Adrie C, Aibiki M, Berg RA, Böttiger BW, Callaway C, Clark RS, Geocadin RG, Jauch EC, Kern KB, Laurent I, Longstreth WT, Jr, Merchant RM, Morley P, Morrison LJ, Nadkarni V, Peberdy MA, Rivers EP, Rodriguez-Nunez A, Sellke FW, Spaulding C, Sunde K, Vanden Hoek T. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. Circulation. 2008;118:2452–2483. - PubMed
-
- Laver S, Farrow C, Turner D, Nolan J. Mode of death after admission to an intensive care unit following cardiac arrest. Intensive Care Med. 2004;30:2126–2128. - PubMed
-
- van Alem AP, Waalewijn RA, Koster RW, de Vos R. Assessment of quality of life and cognitive function after out-of-hospital cardiac arrest with successful resuscitation. Am J Cardiol. 2004;93:131–135. - PubMed
-
- Pusswald G, Fertl E, Faltl M, Auff E. Neurological rehabilitation of severely disabled cardiac arrest survivors. Part II. Life situation of patients and families after treatment. Resuscitation. 2000;47:241–248. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
