

Higher levels of CRP, D-dimer, IL-6, and hyaluronic acid before initiation of antiretroviral therapy (ART) are associated with increased risk of AIDS or death
- PMID: 21592994
- PMCID: PMC3096784
- DOI: 10.1093/infdis/jir134
Higher levels of CRP, D-dimer, IL-6, and hyaluronic acid before initiation of antiretroviral therapy (ART) are associated with increased risk of AIDS or death
Abstract
Background: Substantial morbidity occurs during the first year of antiretroviral therapy (ART) in persons with advanced human immunodeficiency virus (HIV) disease despite HIV suppression. Biomarkers may identify high-risk groups.
Methods: Pre-ART and 1-month samples from an initial ART trial were evaluated for biomarkers associated with AIDS events or death within 1-12 months. Case patients (n = 63) and control patients (n = 126) were 1:2 matched on baseline CD4 cell count, hepatitis status, and randomization date. All had ≥ 1 log(10) HIV RNA level decrease at 1 month.
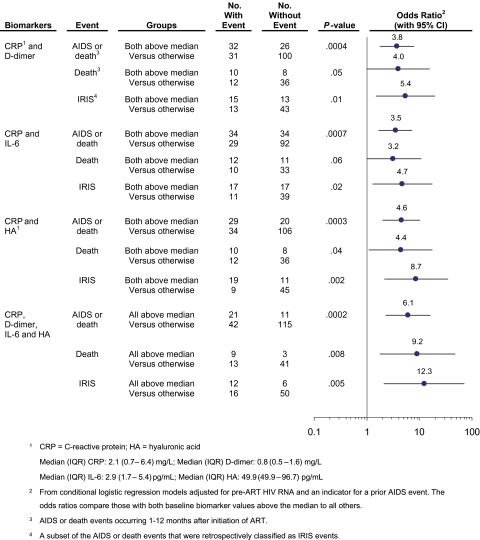
Results: Case patients had more frequent prior AIDS events, compared with control patients (P = .004), but similar HIV RNA levels at baseline. Pre-ART and 1-month C-reactive protein (CRP), D-dimer, and interleukin 6 (IL-6) levels and pre-ART hyaluronic acid (HA) levels were associated with new AIDS events or death (P ≤ .01). Patients who experienced immune reconstitution inflammatory syndrome (IRIS) events had higher pre-ART tumor necrosis factor α (TNF-α) and HIV RNA levels and significant 1-month increases in CRP, D-dimer, IL-6, interleukin 8, CXCL10, TNF-α, and interferon-γ levels, compared with patients who experienced non-IRIS events (P ≤ .03). Individuals with baseline CRP and HA levels above the cohort median (>2.1 mg/L and >50.0 ng/mL, respectively) had increased risk of AIDS or death (OR, 4.6 [95% CI, 2.0-10.3]; P < .001) and IRIS (OR, 8.7 [95% CI, 2.2-34.8] P = .002).
Conclusions: Biomarkers of Inflammation (CRP, IL-6), coagulation (D-dimer), and tissue fibrosis (HA) measured pre-ART and at 1 month are associated with higher risk of AIDS events, IRIS, or death, warranting additional study as risk stratification strategies.
Figures
References
-
- Palella FJ, Baker RK, Moorman AC, et al. Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr. 2006;43:27–34. - PubMed
-
- Palella FJ, Delaney KM, Moorman AC, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. N Engl J Med. 1998;338:853–60. - PubMed
-
- Mocroft A, Ledergerber B, Katlama C, et al. Decline in the AIDS and death rates in the EuroSIDA study: an observational study. Lancet. 2003;362:22–9. - PubMed
-
- Murphy EL, Collier AC, Kalish LA, et al. Highly active antiretroviral therapy decreases mortality and morbidity in patients with advanced HIV disease. Ann Intern Med. 2001;135:17–26. - PubMed
-
- Castelnuovo B, Manabe YC, Kiragga A, Kamya M, Easterbrook P, Kambugu A. Cause-specific mortality and the contribution of immune reconstitution inflammatory syndrome in the first 3 years after antiretroviral therapy initiation in an urban African cohort. Clin Infect Dis. 2009;49:965–72. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
