

IgG4-related hypophysitis: a new addition to the hypophysitis spectrum
- PMID: 21593109
- PMCID: PMC3135201
- DOI: 10.1210/jc.2010-2970
IgG4-related hypophysitis: a new addition to the hypophysitis spectrum
Abstract
Context: Hypophysitis is a chronic inflammation of the pituitary gland that comprises an increasingly complex clinicopathological spectrum. Within this spectrum, lymphocytic and granulomatous hypophysitis are the most common forms, but newer variants have recently been reported.
Objective: The aims of the study were to describe a new patient with IgG4-related hypophysitis, review the published literature, and provide diagnostic criteria.
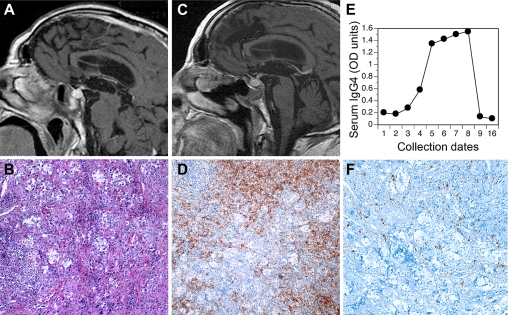
Setting: A 75-yr-old man presented with a 1-yr history of frontal headache. Initial studies revealed panhypopituitarism and a mass in both the sella turcica and the sphenoidal sinus. The patient underwent transphenoidal surgery, initiated high-dose prednisone followed by hormone replacement therapy, and was closely monitored for 3 yr.
Results: Symptoms improved after prednisone, along with shrinkage of the pituitary and sphenoidal masses, but recurred when prednisone dose was lowered. Histopathology showed a marked mononuclear infiltrate in both the pituitary and sphenoidal specimens, mainly characterized by increased numbers of plasma cells. Many of the infiltrating plasma cells (>10 per high-power field) were IgG4-positive. Review of the literature identified 11 cases of IgG4-related hypophysitis (two diagnosed based on pituitary histopathology).
Conclusions: We describe the first Caucasian patient with biopsy-proven IgG4-related hypophysitis and provide classification criteria for this disease.
Figures
References
-
- Howlett TA, Levy MJ, Robertson IJ. 2010. How reliably can autoimmune hypophysitis be diagnosed without pituitary biopsy. Clin Endocrinol (Oxf) 73:18–21 - PubMed
-
- Blansfield JA, Beck KE, Tran K, Yang JC, Hughes MS, Kammula US, Royal RE, Topalian SL, Haworth LR, Levy C, Rosenberg SA, Sherry RM. 2005. Cytotoxic T-lymphocyte-associated antigen-4 blockage can induce autoimmune hypophysitis in patients with metastatic melanoma and renal cancer. J Immunother 28:593–598 - PMC - PubMed
-
- Tebben PJ, Atkinson JL, Scheithauer BW, Erickson D. 2007. Granulomatous adenohypophysitis after interferon and ribavirin therapy. Endocr Pract 13:169–175 - PubMed
-
- Caturegli P, Newschaffer C, Olivi A, Pomper MG, Burger PC, Rose NR. 2005. Autoimmune hypophysitis. Endocr Rev 26:599–614 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
