

Prolonged Tpeak-to-tend interval on the resting ECG is associated with increased risk of sudden cardiac death
- PMID: 21593198
- PMCID: PMC3157547
- DOI: 10.1161/CIRCEP.110.960658
Prolonged Tpeak-to-tend interval on the resting ECG is associated with increased risk of sudden cardiac death
Abstract
Background: Early studies indicate that prolongation of the interval between the peak and the end of the T wave (Tpeak to Tend [TpTe]) on the 12-lead ECG is a marker of ventricular arrhythmogenesis. However, community-based studies have not been conducted.
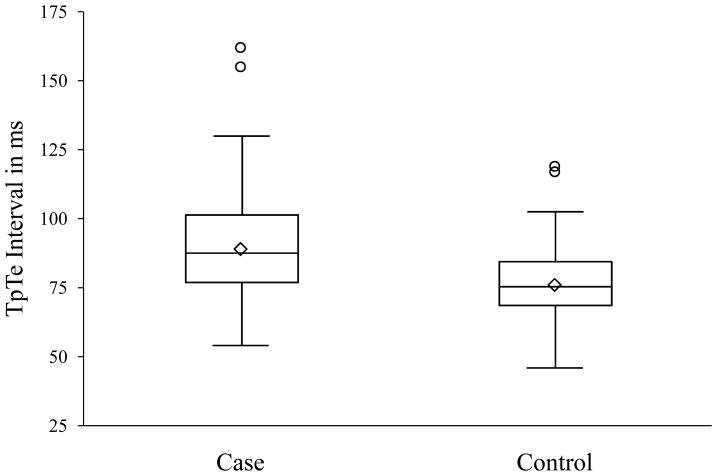
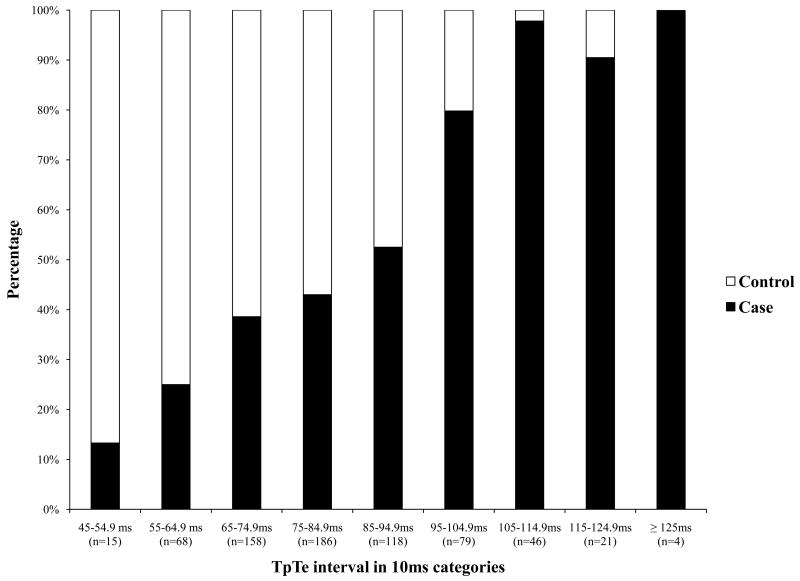
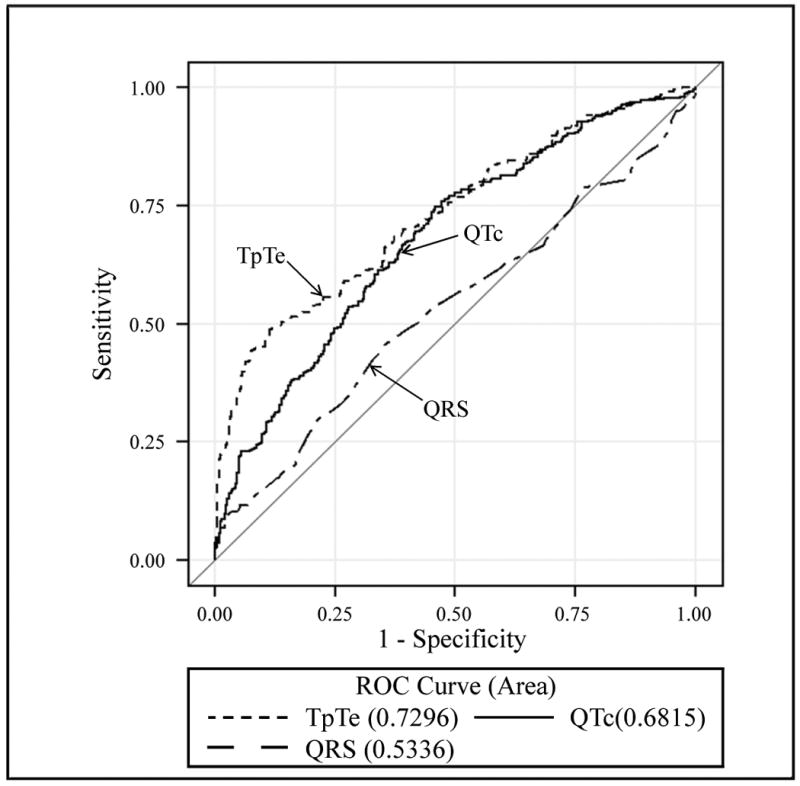
Methods and results: TpTe and other ECG predictors were evaluated in the ongoing Oregon Sudden Unexpected Death Study based in the Portland, Oregon, metropolitan area using a case-control design. Cases of sudden cardiac death (SCD) (n = 353; mean age, 66.6 years; 95% CI, 65.1 to 68.1 years; 67% men) were compared with living controls with coronary artery disease (n = 342; mean age, 64.7 years; 95% CI, 63.4 to 66.0 years; 69% men) from the same region. Analysis of TpTe and selected ECG intervals was limited to sinus rhythm 12-lead ECGs. For cases, these were obtained before and unrelated to SCD. Independent-samples t tests and multiple logistic regression were used. Mean TpTe was significantly greater in cases (89.4 ms; 95% CI, 87.7 to 91.2 ms; P < 0.0001) than in controls (76.1 ms; 95% CI, 74.8 to 77.4 ms). The other ECG intervals (corrected QT interval [QTc], QRS duration [QRSD], and TpTe/QT ratio) also were significantly prolonged among cases versus controls (P ≤ 0.01). TpTe remained a significant predictor of SCD after adjusting for age, sex, QTc, QRSD, and left ventricular function. Odds of SCD increased more with a 1-SD increase in TpTe (12 ms) among subjects with prolonged QRSD (odds ratio, 3.49; 95% CI, 2.06 to 5.91) than with a 1-SD increase in TpTe among subjects with normal QRSD (odds ratio, 1.96; 95% CI, 1.65 to 2.32). TpTe remained significantly associated with SCD in subjects with normal QTc.
Conclusions: Prolongation of the TpTe interval measured in lead V5 was independently associated with SCD, with particular utility when the QTc was normal or not measurable because of prolonged QRSD.
Conflict of interest statement
Figures
Comment in
-
Letter by Opthof et al regarding article, "Prolonged Tpeak to tend interval on the resting electrocardiogram is associated with increased risk of sudden cardiac death".Circ Arrhythm Electrophysiol. 2011 Dec;4(6):e87; author reply e88. doi: 10.1161/CIRCEP.111.965566. Circ Arrhythm Electrophysiol. 2011. PMID: 22203666 No abstract available.
References
-
- Fishman GI, Chugh SS, Dimarco JP, Albert CM, Anderson ME, Bonow RO, Buxton AE, Chen PS, Estes M, Jouven X, Kwong R, Lathrop DA, Mascette AM, Nerbonne JM, O'Rourke B, Page RL, Roden DM, Rosenbaum DS, Sotoodehnia N, Trayanova NA, Zheng ZJ. Sudden cardiac death prediction and prevention: report from a National Heart, Lung, and Blood Institute and Heart Rhythm Society Workshop. Circulation. 2010;122:2335–2348. - PMC - PubMed
-
- Corrado D, Thiene G, Pennelli N. Sudden death as the first manifestation of coronary artery disease in young people (less than or equal to 35 years) Eur Heart J. 1988;9:139–144. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
