

Biomarkers of cobalamin (vitamin B-12) status in the epidemiologic setting: a critical overview of context, applications, and performance characteristics of cobalamin, methylmalonic acid, and holotranscobalamin II
- PMID: 21593511
- PMCID: PMC3174853
- DOI: 10.3945/ajcn.111.013441
Biomarkers of cobalamin (vitamin B-12) status in the epidemiologic setting: a critical overview of context, applications, and performance characteristics of cobalamin, methylmalonic acid, and holotranscobalamin II
Abstract
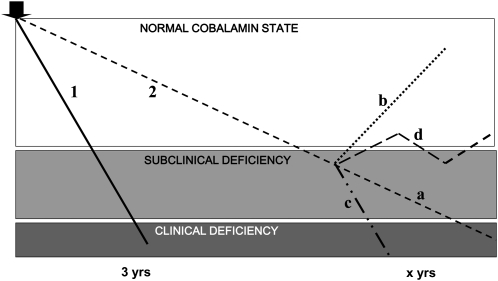
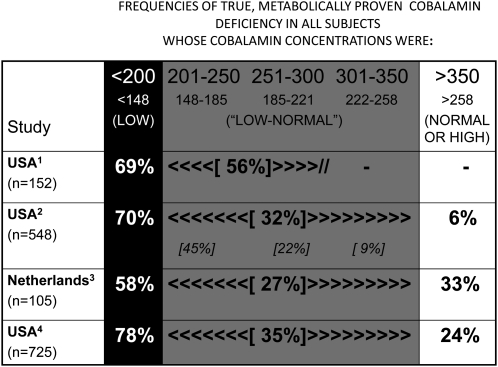
Cobalamin deficiency is relatively common, but the great majority of cases in epidemiologic surveys have subclinical cobalamin deficiency (SCCD), not classical clinical deficiency. Because SCCD has no known clinical expression, its diagnosis depends solely on biochemical biomarkers, whose optimal application becomes crucial yet remains unsettled. This review critically examines the current diagnostic concepts, tools, and interpretations. Their exploration begins with understanding that SCCD differs from clinical deficiency not just in degree of deficiency but in fundamental pathophysiology, causes, likelihood and rate of progression, and known health risks (the causation of which by SCCD awaits proof by randomized clinical trials). Conclusions from SCCD data, therefore, often may not apply to clinical deficiency and vice versa. Although many investigators view cobalamin testing as unreliable, cobalamin, like all diagnostic biomarkers, performs satisfactorily in clinical deficiency but less well in SCCD. The lack of a diagnostic gold standard limits the ability to weigh the performance characteristics of metabolic biomarkers such as methylmalonic acid (MMA) and holotranscobalamin II, whose specificities remain incompletely defined outside their relations to each other. Variable cutoff selections affect diagnostic conclusions heavily and need to be much better rationalized. The maximization of reliability and specificity of diagnosis is far more important today than the identification of ever-earlier stages of SCCD. The limitations of all current biomarkers make the combination of ≥2 test result abnormalities, such as cobalamin and MMA, the most reliable approach to diagnosing deficiency in the research setting; reliance on one test alone courts frequent misdiagnosis. Much work remains to be done.
Figures
References
-
- Carmel R. The disappearance of cobalamin absorption testing: a critical diagnostic loss. J Nutr 2007;137:2481–4 - PubMed
-
- Savage DG, Lindenbaum J, Stabler SP, Allen RH. Sensitivity of serum methylmalonic acid and total homocysteine determinations for diagnosing cobalamin and folate deficiencies. Am J Med 1994;96:239–46 - PubMed
-
- Chanarin I. The megaloblastic anaemias, 2nd ed. Oxford, United Kingdom: Blackwell Scientific Publishing, 1979
-
- Cox EV, White AM. Methylmalonic acid excretion: index of vitamin B12 deficiency. Lancet 1962;2:853–6 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
