

Altered central sensitization in subgroups of women with vulvodynia
- PMID: 21593667
- PMCID: PMC3173591
- DOI: 10.1097/AJP.0b013e31821c98ec
Altered central sensitization in subgroups of women with vulvodynia
Abstract
Objective: To investigate the clinical correlates of central nervous system alterations among women with vulvodynia. Altered central sensitization has been linked to dysfunction in central nervous system-inhibitory pathways (e.g., γ-aminobutyric acidergic), and metrics of sensory adaptation, a centrally mediated process that is sensitive to this dysfunction, could potentially be used to identify women at risk of treatment failure using conventional approaches.
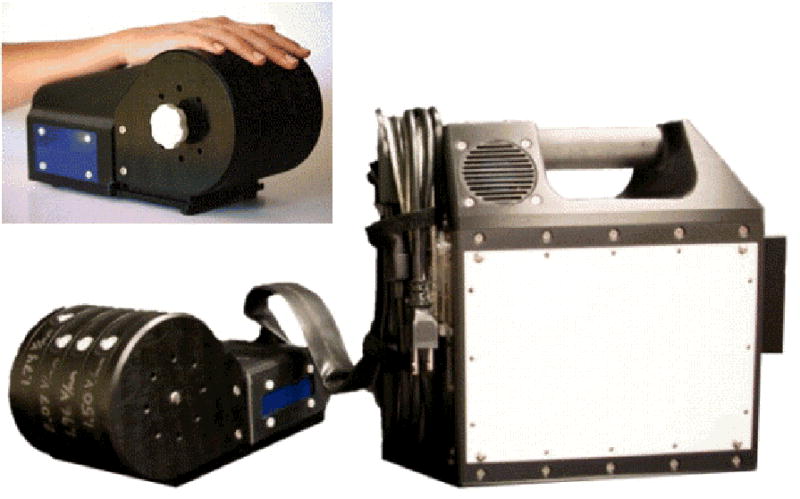
Methods: Twelve women with vulvodynia and 20 age-matched controls participated in this study, which was conducted by sensory testing of the right hand's index and middle fingers. The following sensory precepts were assessed: (1) vibrotactile detection threshold; (2) amplitude discrimination capacity (defined as the ability to detect differences in intensity of simultaneously delivered stimuli to 2 fingers); and (3) a metric of adaptation (determined by the impact that applying conditioning stimuli have on amplitude discriminative capacity).
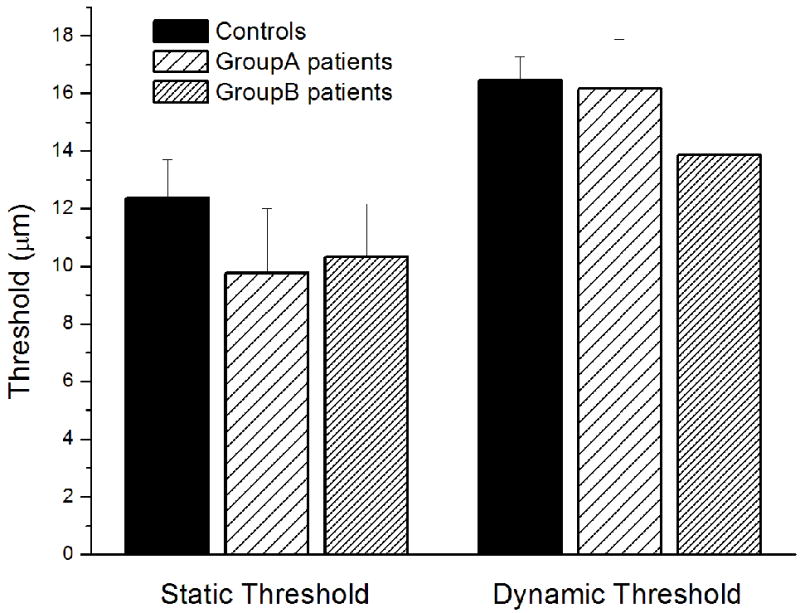
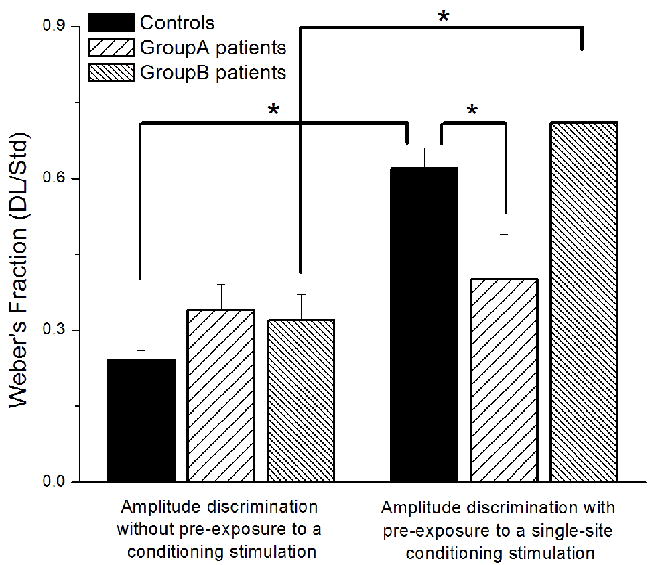
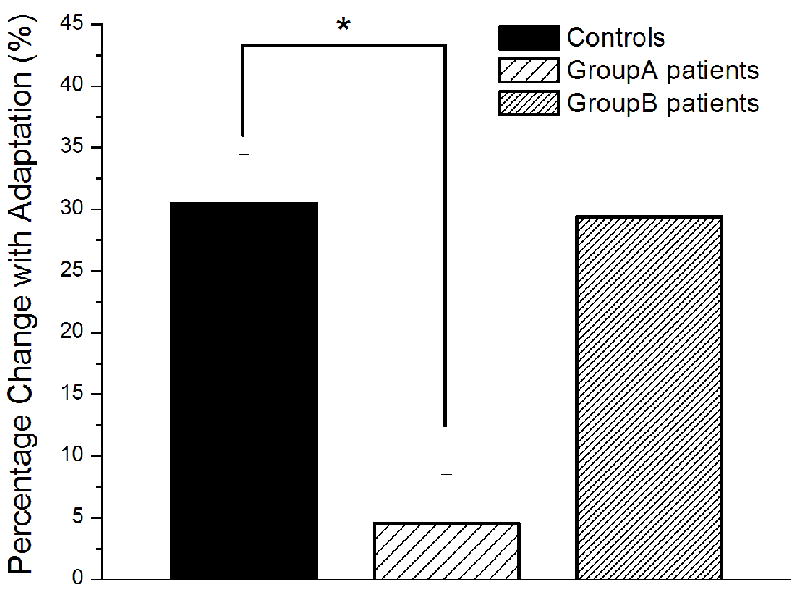
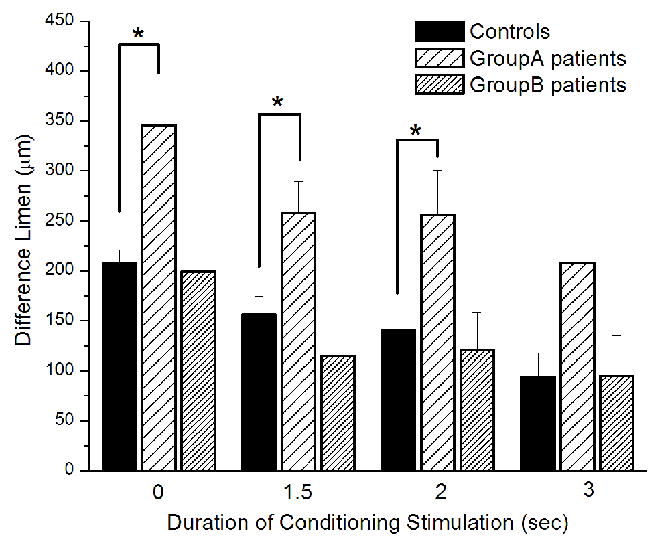
Results: Participants did not differ on key demographic variables, vibrotactile detection threshold, and amplitude discrimination capacity. However, we found significant differences from controls in adaptation metrics in 1 subgroup of vulvodynia patients. Compared with healthy controls and women with a shorter history of pain [n=5; duration (y) = 3.4 ± 1.3], those with a longer history [n=7; duration (y) = 9.3 ± 1.4)] were found to be less likely to have adaptation metrics similar to control values.
Discussion: Chronic pain is thought to lead to altered central sensitization, and adaptation is a centrally mediated process that is sensitive to this condition. This report suggests that similar alterations exist in a subgroup of vulvodynia patients.
Figures
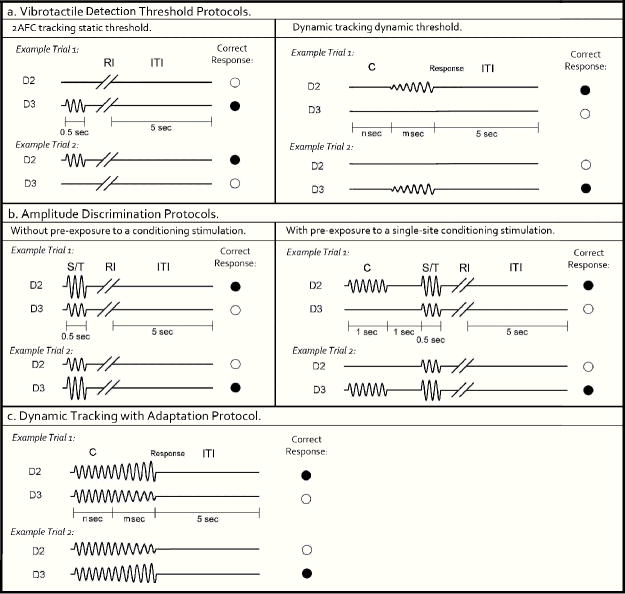
Vibrotactile detection threshold protocols. Left panel: 2AFC tracking protocol: In each trial, a 25 Hz vibrotactle test stimulus was delivered to either D2 or D3 for 0.5 sec, followed by a subject response interval (RI). Subject was prompted to select the skin site that perceived the stimulus. A 5 sec inter-trial interval (ITI) intervened between stimulus response and onset of the next trial. Right panel: Dynamic tracking protocol: A delay period (n sec = 0, 1.5, 2 or 3 sec) without any stimulation was applied. After the initial delay, a 25 Hz vibrotactile stimulus was delivered to either D2 or D3. The amplitude of the stimulus was initiated from zero and increased in steps of 2 μm/sec. The stimulation was terminated with subject response to the perceived stimulus.
Amplitude discrimination protocols. Left panel: Amplitude discrimination at baseline: Two 25 Hz vibrotactile stimuli, the standard (S) and test (T), were delivered simultaneously for 0.5 sec. Subject was asked to choose the stimulus that was perceptually larger. Right panel: Amplitude discrimination task with pre-exposure to conditioning stimulation. A 25 Hz conditioning stimulus was delivered 1 sec prior to the presentation of the test and standard stimuli.
Dynamic tracking with adaptation protocol: Two identical 25 Hz vibrotactile stimuli were delivered simultaneously for a fixed interval (n sec = 0, 1.5, 2, or 3 sec). After the initial constant stimulus period, the amplitude of the two stimuli were dynamically increased/decreased, in steps of 25 μm/sec. Stimulation was terminated with subject response to the location at which the most intense stimulus was delivered.
References
-
- Danby CS, Margesson LJ. Approach to the diagnosis and treatment of vulvar pain. Dermatol Ther. 2010;23:485–504. - PubMed
-
- Harlow BL, Wise LA, Stewart EG. Prevalence and predictors of chronic lower genital tract discomfort. Am J Obstet Gynecol. 2001;185:545–550. - PubMed
-
- Giesecke J, Reed BD, Haefner HK, et al. Quantitative sensory testing in vulvodyniapatients and increased peripheral pressure pain sensitivity. Obstet Gynecol. 2004;104:126–133. - PubMed
-
- Gunter J. Vulvodynia: New Thoughts on a devastating condition. Obstet Gynecol Surv. 2007;62:812–819. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
