

Comparison of glucostatic parameters after hypocaloric diet or bariatric surgery and equivalent weight loss
- PMID: 21593800
- PMCID: PMC3670603
- DOI: 10.1038/oby.2011.134
Comparison of glucostatic parameters after hypocaloric diet or bariatric surgery and equivalent weight loss
Abstract
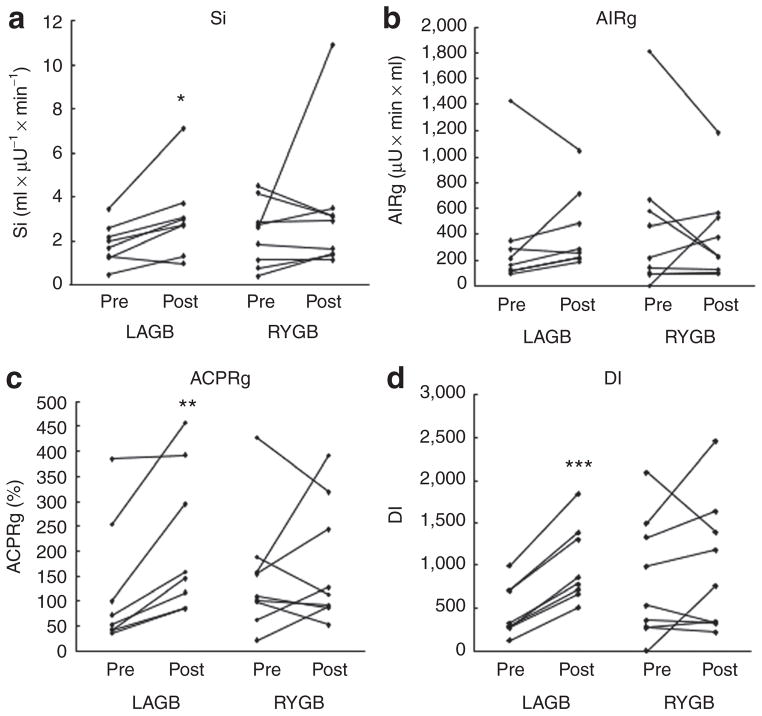
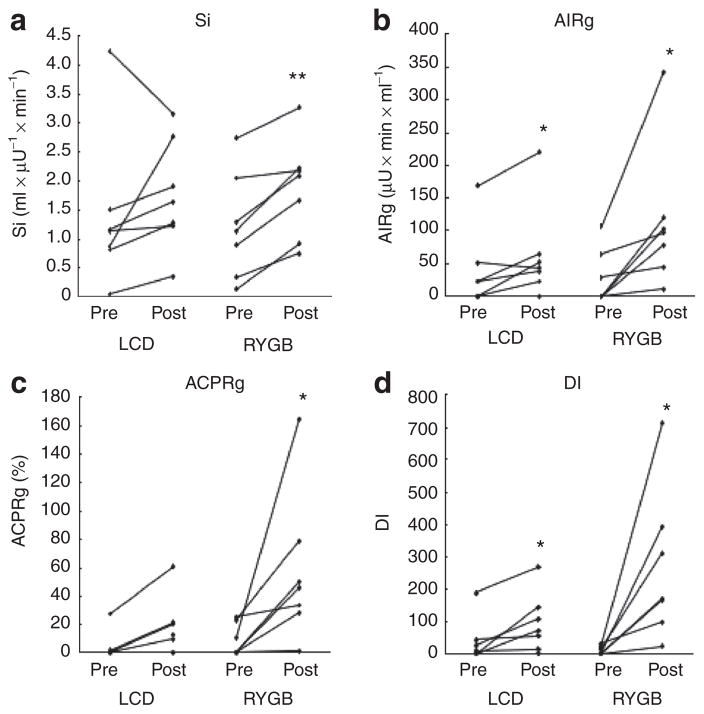
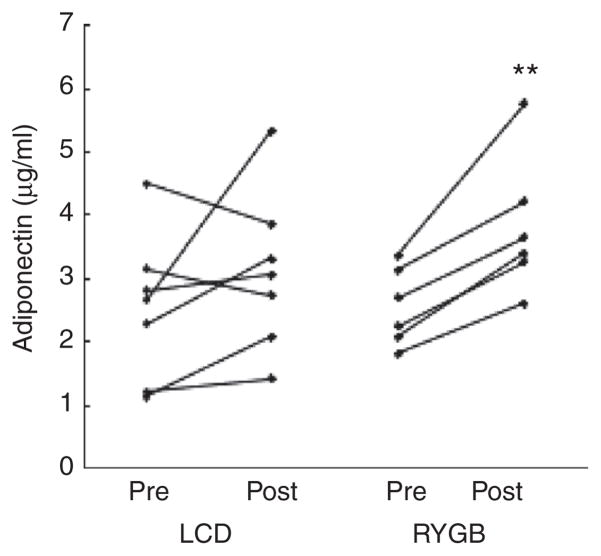
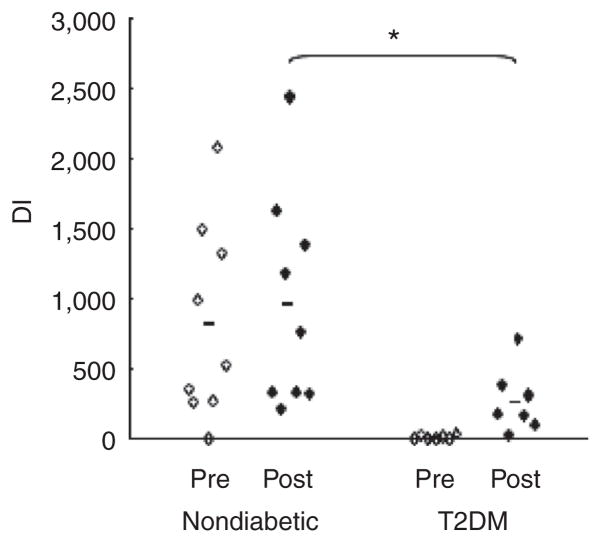
Weight-loss independent mechanisms may play an important role in the improvement of glucose homeostasis after Roux-en-Y gastric bypass (RYGB). The objective of this analysis was to determine whether RYGB causes greater improvement in glucostatic parameters as compared with laparoscopic adjustable gastric banding (LAGB) or low calorie diet (LCD) after equivalent weight loss and independent of enteral nutrient passage. Study 1 recruited participants without type 2 diabetes mellitus (T2DM) who underwent LAGB (n = 8) or RYGB (n = 9). Study 2 recruited subjects with T2DM who underwent LCD (n = 7) or RYGB (n = 7). Insulin-supplemented frequently-sampled intravenous glucose tolerance test (fsIVGTT) was performed before and after equivalent weight reduction. MINMOD analysis of insulin sensitivity (Si), acute insulin response to glucose (AIRg) and C-peptide (ACPRg) response to glucose, and insulin secretion normalized to the degree of insulin resistance (disposition index (DI)) were analyzed. Weight loss was comparable in all groups (7.8 ± 0.4%). In Study 1, significant improvement of Si, ACPRg, and DI were observed only after LAGB. In Study 2, Si, ACPRg, and plasma adiponectin increased significantly in the RYGB-DM group but not in LCD. DI improved in both T2DM groups, but the absolute increase was greater after RYGB (258.2 ± 86.6 vs. 55.9 ± 19.9; P < 0.05). Antidiabetic medications were discontinued after RYGB contrasting with 55% reduction in the number of medications after LCD. No intervention affected fasting glucagon-like peptide (GLP)-1, peptide YY (PYY) or ghrelin levels. In conclusion, RYGB produced greater improvement in Si and DI compared with diet at equivalent weight loss in T2DM subjects. Such a beneficial effect was not observed in nondiabetic subjects at this early time-point.
Figures
References
-
- Yach D, Stuckler D, Brownell KD. Epidemiologic and economic consequences of the global epidemics of obesity and diabetes. Nat Med. 2006;12:62–66. - PubMed
-
- Wadden TA. Treatment of obesity by moderate and severe caloric restriction. Results of clinical research trials. Ann Intern Med. 1993;119:688–693. - PubMed
-
- Cummings DE. Endocrine mechanisms mediating remission of diabetes after gastric bypass surgery. Int J Obes (Lond) 2009;33 (Suppl 1):S33–S40. - PubMed
-
- Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724–1737. - PubMed
-
- Pories WJ, MacDonald KG. The surgical treatment of morbid obesity. Curr Opin Gen Surg. 1993:195–205. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
