

Trans-apical beating-heart implantation of neo-chordae to mitral valve leaflets: results of an acute animal study
- PMID: 21596577
- PMCID: PMC3241122
- DOI: 10.1016/j.ejcts.2011.03.058
Trans-apical beating-heart implantation of neo-chordae to mitral valve leaflets: results of an acute animal study
Abstract
Objective: Trans-apical beating-heart implantation of neo-chordae is yet an experimental procedure for mitral valve (MV) repair. We aimed to assess the performance of a new device in an acute animal study.
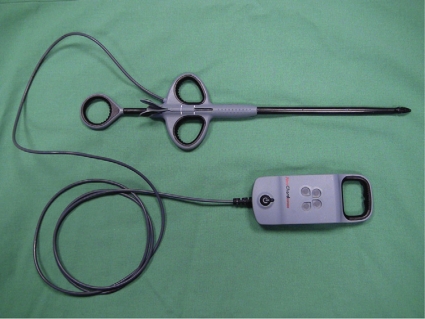
Methods: A total of four domestic adolescent pigs were used as an acute model. The MV was assessed on the beating heart through a conventional trans-apical access. The NeoChord DS1000 device was used to implant polytetrafluoroethylene (PTFE) sutures to the MV leaflets. Procedural performance of the device was assessed and completed with surgical workflow analysis.
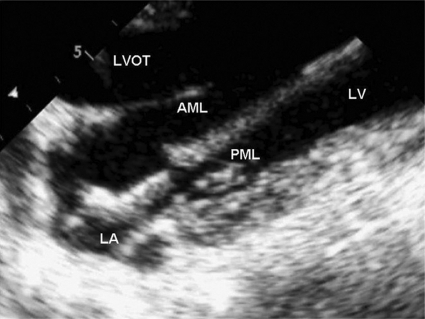
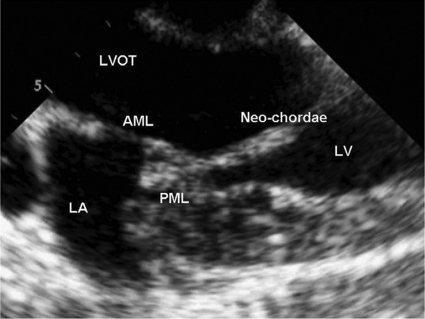
Results: Overall 57 implantations using epicardial echocardiography guidance were performed (mean 14.3 implantations per animal). The MV leaflets were successfully grasped every second attempt (mean 2.3±1.9) with no difference between the anterior and the posterior leaflet. A significant difference between an 'expert' surgeon (n>20 implantations) and beginner surgeon was detected with regard to the duration for successful leaflet grasping (65±73 vs 127±105 s; p=0.02) and the overall duration for implantation (130±86 vs 230±119 s; p=0.002). Gross anatomy did not show major tear of leaflets. There were no device-related technical problems.
Conclusion: The NeoChord DS1000 device for trans-apical beating-heart implantation of neo-chordae to the MV valve showed a high procedural success. A significant difference between an expert and beginner surgeon was detected, which emphasizes the importance of training before introduction of this new technique into clinical practice. Surgical workflow analysis proved to be a valuable tool to assess the performance of this new technique.
Figures
References
-
- Braunberger E, Deloche A, Berrei A, Abdallah F, Celestin JA, Meimoun P, Chatellier G, Chauvaud S, Fabiani JN, Carpentier A. Very long-term results (more than 20 years) of valve repair with Carpentier’s techniques in nonrheumatic mitral valve insufficiency. Circulation. 2001;104:I8–11. - PubMed
-
- David TE, Ivanov J, Armstrong S, Christie D, Rakowski H. A comparison of outcomes of mitral valve repair for degenerative disease with posterior, anterior, and BL prolapse. J Thorac Cardiovasc Surg. 2005;130:1242–9. - PubMed
-
- Gillinov AM, Cosgrove DM, Blackstone EH, Diaz R, Arnold JH, Lytle BW, Smedira NG, Sabik JF, McCarthy PM, Loop FD. Durability of mitral valve repair for degenerative disease. J Thorac Cardiovasc Surg. 1998;116:734–43. - PubMed
-
- Seeburger J, Borger MA, Doll N, Walther T, Passage J, Falk V, Mohr FW. Comparison of outcomes of minimally invasive mitral valve surgery for posterior, anterior, and bileaflet prolapse. Eur J Cardiothorac Surg. 2009;36:532–8. - PubMed
-
- Frater RW, Vetter HO, Zussa C, Dahm M. Chordal replacement in mitral valve repair. Circulation. 1990;82:IV125–30. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
