

Surgery with disc prosthesis versus rehabilitation in patients with low back pain and degenerative disc: two year follow-up of randomised study
- PMID: 21596740
- PMCID: PMC3100911
- DOI: 10.1136/bmj.d2786
Surgery with disc prosthesis versus rehabilitation in patients with low back pain and degenerative disc: two year follow-up of randomised study
Abstract
Objective: To compare the efficacy of surgery with disc prosthesis versus non-surgical treatment for patients with chronic low back pain.
Design: A prospective randomised multicentre study.
Setting: Five university hospitals in Norway.
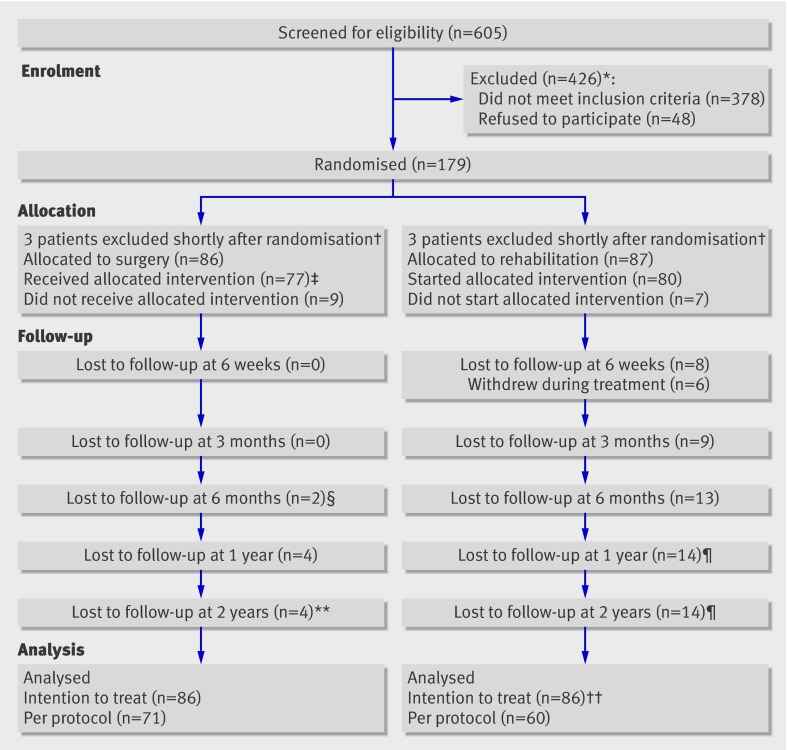
Participants: 173 patients with a history of low back pain for at least one year, Oswestry disability index of at least 30 points, and degenerative changes in one or two lower lumbar spine levels (86 patients randomised to surgery). Patients were treated from April 2004 to September 2007.
Interventions: Surgery with disc prosthesis or outpatient multidisciplinary rehabilitation for 12-15 days.
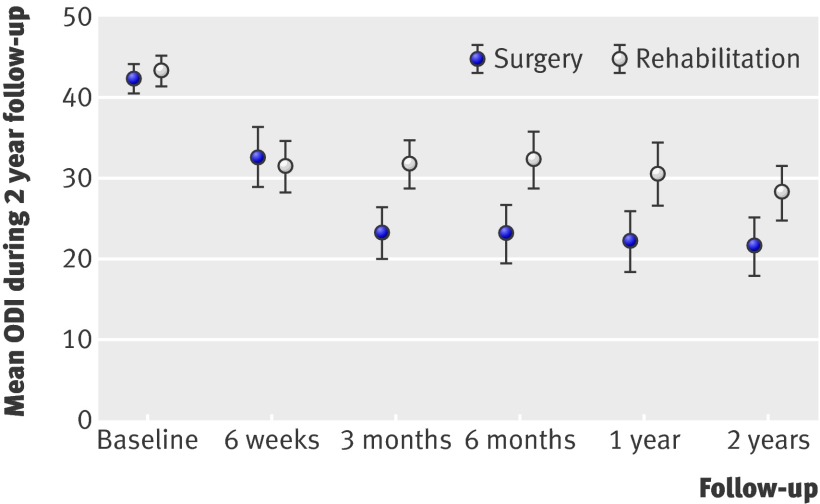
Main outcome measures: The primary outcome measure was the score on the Oswestry disability index after two years. Secondary outcome measures were low back pain, satisfaction with life (SF-36 and EuroQol EQ-5D), Hopkins symptom check list (HSCL-25), fear avoidance beliefs (FABQ), self efficacy beliefs for pain, work status, and patients' satisfaction and drug use. A blinded independent observer evaluated scores on the back performance scale and Prolo scale at two year follow-up.
Results: The study was powered to detect a difference of 10 points on the Oswestry disability index between the groups at two years. At two years there was a mean difference of -8.4 points (95% confidence interval -13.2 to -3.6) in favour of surgery. In the analysis of prespecified secondary outcomes, there were significant differences in favour of surgery for low back pain (mean difference -12.2, -21.3 to -3.1), patients' satisfaction (63% (n = 46) v 39% (n = 26)), SF-36 physical component score (mean difference 5.8, 2.5 to 9.1), self efficacy for pain (mean difference 1.0, 0.2 to 1.9), and the Prolo scale (mean difference 0.9, 0.1 to 1.6). There were no significant differences in return to work, SF-36 mental component score, EQ-5D, fear avoidance beliefs, Hopkins symptom check list, drug use, and the back performance scale. One serious complication of leg amputation occurred during surgical revision of a polyethylene dislodgement. The drop-out rate was 20% (34) and the crossover rate was 6% (5).
Conclusions: Surgical intervention with disc prosthesis for chronic low back pain resulted in a significantly greater improvement in the Oswestry score compared with rehabilitation, but this improvement did not clearly exceed the prespecified minimally important clinical difference between groups of 10 points, and the data are consistent with a wide range of differences between the groups, including values well below 10 points. The potential risks of surgery and the substantial amount of improvement experienced by a sizeable proportion of the rehabilitation group also have to be incorporated into overall decision making. Trial registration NCT 00394732.
Trial registration: ClinicalTrials.gov NCT00394732.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Total disc replacement for chronic low back pain.BMJ. 2011 May 19;342:d2745. doi: 10.1136/bmj.d2745. BMJ. 2011. PMID: 21596739 No abstract available.
-
Guidance on minimally important clinical difference and trial size is needed.BMJ. 2011 Jul 25;343:d4375. doi: 10.1136/bmj.d4375. BMJ. 2011. PMID: 21788268 No abstract available.
-
Besserer Schmerz- und Funktionalitätsstatus durch Implantation einer künstlichen Bandscheibe im Vergleich zur konservativen Therapie.Praxis (Bern 1994). 2011 Sep 21;100(19):1199-200. doi: 10.1024/1661-8157/a000675. Praxis (Bern 1994). 2011. PMID: 21938717 German. No abstract available.
-
Surgery with disc prosthesis may produce better outcomes than multidisciplinary rehabilitation for patients with chronic low back pain.J Physiother. 2011;57(4):257. doi: 10.1016/S1836-9553(11)70058-3. J Physiother. 2011. PMID: 22093126
-
[Operations].Orthopade. 2012 Dec;41(12):991. doi: 10.1007/s00132-012-1976-x. Orthopade. 2012. PMID: 23192730 German. No abstract available.
References
-
- Waddell G. The back pain revolution. 2nd ed. Churchill Livingstone, 2004.
-
- Fritzell P, Hagg O, Wessberg P, Nordwall A, for the Swedish Lumbar Spine Study Group. 2001 Volvo Award Winner in Clinical Studies: lumbar fusion versus nonsurgical treatment for chronic low back pain: a multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine 2001;26:2521-32. - PubMed
-
- Brox JI, Sorensen R, Friis A, Nygaard O, Indahl A, Keller A, et al. Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-21. - PubMed
-
- Brox JI, Reikeras O, Nygaard O, Sorensen R, Indahl A, Holm I, et al. Lumbar instrumented fusion compared with cognitive intervention and exercises in patients with chronic back pain after previous surgery for disc herniation: a prospective randomized controlled study. Pain 2006;122:145-55. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous